















The Role of Disabled Persons in Overcoming Rural Poverty in Andhra Pradesh, India: Enabling the ‘Poorest of the Poor’
In February/March, 2002, I (David Werner) was invited to India as a consultant to a comprehensive program to reduce poverty throughout the rural area of Andhra Pradesh.
Aware that many large-scale, top-down programs to combat poverty have failed to reach the most destitute and marginalized persons—and consequently have marginalized them more—the designers of the Andhra Pradesh Rural Poverty Reduction Program are taking a different approach. The focus will be on the most needy and vulnerable groups in rural areas (where 2/3 of the state’s 76 million population live).
These “most vulnerable” groups include:
-
the “poorest of the poor,” including the jobless and homeless
-
those belonging to the lowest “untouchable” caste (Dalits)
-
tribal and nomadic populations
-
women (especially widows and single mothers)
-
children (especially girls)
-
the indigent elderly and infirm
-
disabled persons.
Following the principles of participation and empowerment, the plan is for representatives from all of these most vulnerable groups to play a leading role in the development and implementation of the poverty reduction strategy. This may sound like common sense. But in a land where class, caste, and gender hierarchies are so deeply entrenched, achieving effective leadership and a more equal voice for those who have been on the bottom of the pecking order for millennia will be a complex challenge.
The Andhra Pradesh Rural Poverty Reduction Program (APRPRP) is under ordinance of the state government (whose capital is Hyderabad, in east-central India) and financed in large part by the World Bank. However, local non-government organizations (NGOs) are playing a leading role in both the program design and field work.
The disability component of the APRPRP is being facilitated by “Commitments,” a branch of a very capable Indian NGO called the Society for Elimination of Poverty (SERC). Although the Bank would have preferred a more mainstream advisor, Commitments insisted that I (David Werner) be the “independent consultant” to the disability component of the APRPRP. One reason they wanted me was that the self-help books, Disabled Village Children and Nothing About Us Without Us are so widely used in community programs in India.
While in India, I met with several groups that have translated or are translating these books into Telugu, the area’s traditional language. (One result of my visit was to engender more cooperation between the diverse programs working in this field.) Also I found that the Telugu version of Where There Is No Doctor is widely used. And what pleases me more, facilitators of both community based health and rehabilitation training programs are using Helping Health Workers Learn to make their teaching methods more discovery-based and learner-centered.
In-Depth Analytic Survey of Disability Needs in Rural Andhra Pradesh
The Disability Component of the Andhra Pradesh Rural Poverty Reduction Program has many features of Community Based Rehabilitation (CBR). However it also has an essential quality of the Independent Living Movement, in that it tries to open the way for leadership by disabled persons themselves.
Disabled persons played a leading role, even in the planning stage of the program, by conducting the initial survey for an “In-depth Analysis of the Disability Issues” in the state. To oversee the survey, SERC chose the Regional Office of “Action Aid,” an NGO based in the state capital, Hyderabad. Action Aid has a long history of working for the rights and opportunities of marginalized groups, especially disabled persons.
To plan the survey, Action Aid met with disabled activists in Hyderabad, as well as from the rural area. Together they designed a creative, culturally appropriate strategy for conducting the in depth survey. The result was a remarkably sensitive, participatory process with some unique features.
Avoiding the Typical Problems with Surveys. Surveys in which outsiders question people in poor communities have in recent years drawn a lot of criticism. Because they distrust the interviewers or feel humiliated by their questions, too often those interviewed give false or misleading information. Or they tell the interviewers what they think they want to know. When interviewers are pushy, condescending, or insensitive to the sociocultural dynamics of the community, data is even more likely to be invalid.
The communications problems common to surveys were minimized in the Andhra Pradesh disability survey in 3 ways:
- The information gatherers were them selves disabled, giving them insight and making them peers of those primarily being interviewed.
- The information gatherers were specially trained in cross-cultural sensitivity, methods of empowerment, and community mobilization.. (One of the facilitators was none other than my old friend, B. Venkatesh, a blind disability-rights activist who visited PROJIMO many years ago);
- The survey was combined with a dynamicprocess of group building, community awareness raising and collective action.
Recruitment of Interviewers. To recruit the information gatherers, Action Aid carefully screened scores of young, literate, disabled persons, from which they picked a group of 80. In the selection, insight, attitudes, and a humble background were given more weight than academic qualifications. On purpose, the group included persons with a wide range of disabilities. It also included representatives from more vulnerable groups, especially persons of rural origins,women, those from lower castes, including Dalits (untouchables), and persons from religious minorities (Muslims, Christians).
Coverage of the Survey: The study covered 52 villages from 20 mandals (groups of villages) in 15 districts. Locations were selected based on those with the biggest problems and needs. These included:
- interior rural areas (those with the poorest,most deprived and underserved populations)
- homelands of “primitive” tribal groups or"schedule caste” populations (Untouchables, Dalits)
- the driest (unirrigated) least fertile lands
- areas with shortage of drinking water, especially those with high fluoride content (a cause of a widespread disability: fluorosis)
- areas with high unemployment or a large population of peasants who are landless or have very small holdings
- areas with very low literacy rates.
In the survey, all of these factors (and many others) were evaluated in terms of their impact on incidence of disability and influence on disabled persons’ well-being . To survey a village (usually with 1000 to 2000 residents), a team of information gatherers would stay in the village for 5 days, living in the homes of persons with different disabilities. Whenever possible, the team leader would stay in the home of the most severely disabled or marginalized person or family in the village (paying the costs). They would do their best to become a friend of the disabled person, the family, and neighbors, trying to gain insight into their spectrum of problems, while helping to resolve or look for ways of resolving the ones they could.
Humanitarian approach: The study—which was designed around “a rights-based approach to Community Based Rehabilitation (CBR)"—proactively addressed the following areas:
- Rescue planning and protection for the destitute among the disabled persons
- Protection of the rights of “the disabled”
- Education
- Medical integration—care, aids and appliances
- Social reintegration
- Work and income generating opportunities.
But the information gatherers did far more than collect data. They brought disabled people together to discuss their mutual problems and needs. They helped groups of disabled persons begin to form self-help groups, or “sangams.” They conducted awareness raising activities, including public theater, in the villages surveyed. And before leaving the village they organized a kind of “disability pride” march of disabled people and their families.
A complaint about many surveys in and of disadvantaged communities is that they build up people’s expectations, but the promised benefits never arrive. People feel used, deceived, and stop cooperating.
To avoid this, in Andhra Pradesh, the survey included a service component. It brought disabled people and their families together to discuss their needs, learn their legal entitlements, and begin to take organized action. At the same time, it launched a constructive dialogue with the larger community and with village authorities to help open the way for more equal opportunities and more accountability. It also helped the disabled persons gain free access to medical and orthopedic facilities.
Good role models. In many ways, the employment and leadership of disabled persons as key actors in this Andhra Pradesh analytic survey was a groundbreaking approach. The fact that the facilitators were themselves disabled provided excellent role models for the disabled villagers and their families. The methodology deserves dissemination. Fortunately, it is well documented, and much of the community process was video-taped. An important resource.
Meeting with the Information Gatherers
Before the disabled “information gatherers” began to visit the villages, they went through an intensive, highly participatory learning process using methods of group dynamics, confidence building, peer counseling, and “strategies of empowerment.” The sessions involved role plays in which everyone practiced listening to and learn from one another as equals. These methods—drawing on the “pedagogy of liberation” of Paulo Freire—were designed to help them reach out to multiple disadvantaged persons, build their self-esteem, and win their trust, so that those interviewed could gain the self-confidence and trust to speak openly of their true feelings, needs, obstacles, fears, and hopes.
In my meeting with the information gatherers at Action Aid, we started by introducing ourselves and describing the difficulties and challenges we had experienced as disabled persons, from early childhood on, as well as the circumstances and events that had changed our lives for the better. Many of the group had grown up in extreme poverty. Nevertheless, I realized that this group was exceptional, in that all of them had somehow succeeded in finding decent work, gaining self-esteem, and playing a dignified, productive role in society.
The information gatherers described the pervasive social and economic obstacles they had struggled to overcome. For example, one village girl, who belonged to the Dalit (untouchable) caste, described herself as being “triple disadvantaged.” She was: 1) disabled (one leg paralyzed by polio), 2) female, and 3) a Dalit, i.e. born into the “lowest,” most denigrated social caste. Added to all this, she had grown up in a situation of rural poverty. Tellingly, she said that the hardship and social stigma she had suffered for being Dalit was greater than that of being disabled. This comment made clear the importance of looking at disability within the entire sociocultural and economic context.
As I listened to the different members of the study team describe their personal backgrounds and difficulties, I was impressed by how far they had come in terms of coping skills and personal esteem. It was apparent that their being involved in the DPIG survey/analysis—designed to give a voice to rural poor disabled persons—has been an eye-opening and empowering process not only for the disabled persons interviewed, but also for these information gatherers themselves. A true win-win situation.
Most of the disabled information gatherers had not known each other before they were recruited. But in less than a year they had developed a strong sense of camaraderie and solidarity. More than most disabled persons (where the pecking order between different disabilities can be as unkind as that in society as a whole), they reached out to include one another as equals. For example, those who had learned sign language (to interview deaf persons) enthusiastically translated our full discussion into sign, for the 2 participants who were deaf.
‘Sangams’ (Self-Help Groups) as an Entry Point to Poverty Reduction
As a pilot project of the APRPRP, a Community Based Disability Intervention has been introduced in Mahabubnagar District, one of the poorest in Andhra Pradesh. Since 1984 the Commitments team has been working in Mahabubnagar, in community development, poverty reduction, and disability rights. The goal is to empower vulnerable groups by “building participatory and self-managed institutions and developing sustainable livelihood capacities.”
One of the APRPRP approaches to poverty reduction is through the formation and assistance of “sangams” (common interest self help groups) among the most disadvantaged groups (women, Dalits, landless peasants, disabled persons, etc.) at the village level. Through the sangam, people can work together to improve their situation, both socially and economically. They can define their common needs and biggest barriers, and collectively take problem-solving action including income-generating activities.
These “from the bottom up” activities are supplemented by the “from the top down”: APRPRP personnel who try to win cooperation and support from officials at the village, mandal, district, and state level, in matters of schooling, safety, employment, fair wages (or at least legal minimum wages), access to legal entitlements, and basic human rights.
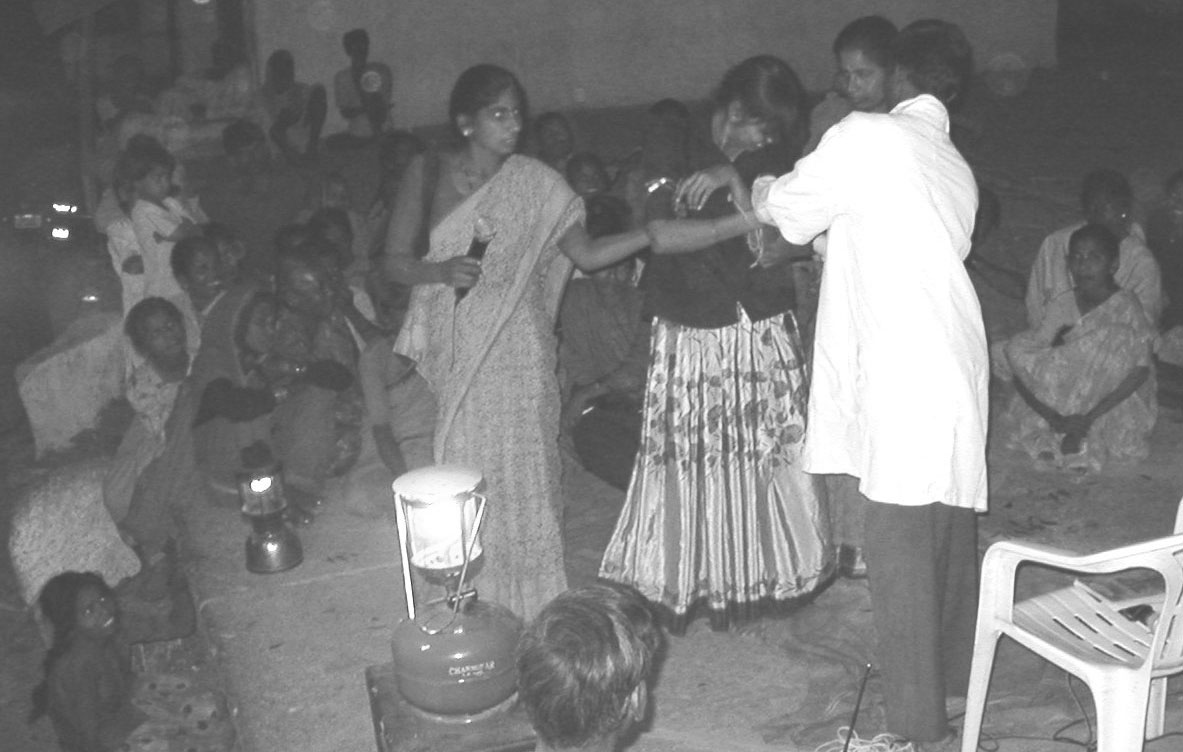
Open-Air Theater to Raise Awareness
History of ‘Vikalangula Sangams’
In 1999, in the small village of Kosgi, Commitments opened a modest Project Office, which doubles as a community rehabilitation and training center. In 6 mandals, the team has helped to start 70 “Vikalangula Sangams” (self-help groups of disabled persons). To help organize and facilitate the initiative, Commitments has trained several “Community Coordinators” (CCs), as well as 20 village activists and social workers, mostly disabled. I was impressed by the dedication and ability of this group. The fact that 3/4 of them are disabled contributes to their understanding of key issues and commitment to empowerment of other disabled persons.
In this, Commitments is to be applauded. In other programs, such leadership by disabled persons is less than common. Even in the (relatively few) Community Based Rehabilitation (CBR) programs in India, seldom do disabled persons play leading roles in program implementation. If this Commitments model of having programs for disabled persons staffed by disabled persons is successfully scaled up within the statewide APRPRP program—as is the plan—it will be a breakthrough of far-reaching significance.
Visits to ‘Disability Sangams’
The program staff (who love acronyms) refer to the Vikalangula Sangams as DCIGs: short for Disability-oriented Common Interest Groups. In smaller villages there is often a single Disability Sangam with 15 to 20 members. At meetings, disabled children and mentally handicapped persons are usually accompany by their parents. (However, I soon discovered, some of the older children play important leadership roles themselves).
Reaching Across Barriers. In the Disability Sangams we visited, members made a conscious effort to reach out and include all disabled persons in the village, whatever their disability or social status. In terms of breaking down entrenched barriers this was a big step forward. Because of their common identity as “disabled persons,” sangam members’ are more willing to reach out to others across the traditional walls of class, caste, gender, and even generation (adults to children). Persons who would otherwise never have spoken to each other and certainly not on an equal level—were beginning to do so. And by doing so, they discover the other things they had in common, apart from disability. In terms of transcending entrenched social barriers, the sangams are real bridge builders.
Fighting for Entitlements. What impressed me most on visiting the sangams was people’s energy and enthusiasm in trying to collectively improve their situation. Nearly all the groups have been making an organized demand for their legal certification and entitlements (which has proved an uphill battle). They have worked to get disabled children into schools (which is their legal right, but not easy). And with the help of Commitments, they are striving to get necessary medical care, surgery, and assistive devices they need.
Winning Respect in the Community. In all the Disability Sangams we visited, members said that one of their biggest accomplishments so far has been their campaign to be treated with respect. Awareness raising activities, including educational street theatre, have reportedly had an impact on changing how people see disability.
“Now people don’t call us ’the lame boy’ or ’the blind girl’ but address us by our real names,” children said proudly.
When I heard this, from my own childhood I recalled how important “names” can be. I explained to the group that as a boy (because I limped due to a hereditary muscular atrophy) my classmates nicknamed me “Rickets.” I still cringe at the memory! Alas, at that time and place there was no Vikalangula Sangam to provide group support or raise community awareness.
Neighborhood Houses. Many Disability Sangams were eager to start their own “neighborhood house.” They envisioned this as a place where disabled people could meet and exchange ideas, organize activities, master new skills, assist one another with therapy, and learn from visiting rehab professionals. Most important, they saw the Neighborhood House as a place where disabled people can play a visible, pro-active role in the community.
Some of the sangams have applied to Commitments for financial help in setting up a neighborhood house. Two groups were so eager that they have rented a building or acquired donated land, even before Commitments had responded to their request.
Visiting Gundmal: Déjà vu—PROJIMO Makes it to India
Our first visit was to the Aruna Vikalangula Sangam in Gundmal village. The Sangam President is a 16-year-old schoolboy who has one leg withered by polio. Most of the sangam’s members are, in fact, school-aged children. The rest are adults of every age, with diverse disabilities, mostly physical.
The young Gundmal group told us excitedly about their new “Neighborhood Rehabilitation House,” an old building they were loaned by the village panchyat (community council) and are creatively adapting. They were obviously proud of it and were eager to take us there. Our visit coordinator said we were pressed for time, but I begged to see the House, and he agreed.
As we approached the Neighborhood House, I had a sudden feeling of déjà vu. In front of the old building, and inside, the youths had built a variety of rustic playground and rehabilitation equipment. These included parallel bars made from bamboo poles and forked sticks, a simple pressed-earth ramp for easy access, a swing made with an old car tire, a large barrel padded with foam rubber for physical therapy, and an arm-exercise device made with a wheelchair wheel mounted on a wall. All looked disconcertingly familiar.
“Where did you get the ideas to make all this local, low-cost equipment?” I asked.
“From a book somebody gave us called Village Disabled Children,” answered one of the disabled youths. When the head of Commitments told him I was the author of the book (actually titled Disabled Village Children), his jaw fell open with surprise. From that moment on the whole group welcomed me like an old friend.
Visiting Hakeempet: Exploring Alternatives to School
The next day we visited the Sudha Chandran Vikalangula Sangam in Hakeempet village. Here the dynamics were quite different. Most of the children in the sangam were developmentally delayed. Suggested explanations for this high incidence of mental retardation ranged from consanguineous marriages (inbreeding), to pesticides or other chemical contaminants, to the prevalence of premature birth due to the high rates of malnutrition and anemia of pregnant women. (In rural India rates of anemia in women of child bearing age run as high as 90%.)
In our discussion, it became clear that many of these mentally slow children suffered from harsh rejection and exclusion, sometimes even within their own families.
For example, one 11-year-old mildly retarded girl at the meeting was very withdrawn and morose (and very thin). Since her mother had died 3 years before, she lived with her father, who was also mentally a bit slow. He brought her to the sangam meetings only because the group urged him to do so. The girl could talk, but her father would not let her speak for herself. He said he had not senther to school or sought any kind of help for her because she was “totally useless.”
Other parents had better reasons for not sending their children to school. For mentally slow children, they said, schooling was cruel. Mothers said they had tried to get their children into the local primary school, but with frustrating results. Even when the children were accepted, teachers had little patience with them. They scolded or humiliated them in front of the other children, who learned similar behavior from their teachers.
At the Sangam meeting there was an angry looking mildly retarded 13 year old boy named Ram, who sat on the floor all hunched into a ball, scowling. Ram’s mother said she had tried several times to place him in school. But after a few days he had always run away. Now the boy flatly refused to go, even when she threatened to beat him.
This led to an eye-opening discussion as to whether school was always the best option for the slow learning child, especially if teachers and other children fail to treat them with respect or help them learn in a supportive way at their own pace.
I reflected on our experience in rural Mexico. Sometimes a mentally retarded child is happier, learns more, and feels he or she is making a greater contribution by helping his or her parents in the farm work, or by doing a simple, if repetitive job.
We concluded that there is need for flexibility and common sense, both in questions of schooling, and of “child labor.” To simply say, “Schooling is good,” and “Child labor is bad” is simplistic. We should ask ourselves, “Where does the the child seem happiest, learn most, and best develop his or her potential?'
Whether, under the circumstances, the parents in Hakeempet should try to get their mentally retarded children into the school, remained unclear. What was very clear was that these children needed an opportunity to play and interact and learn with other children.
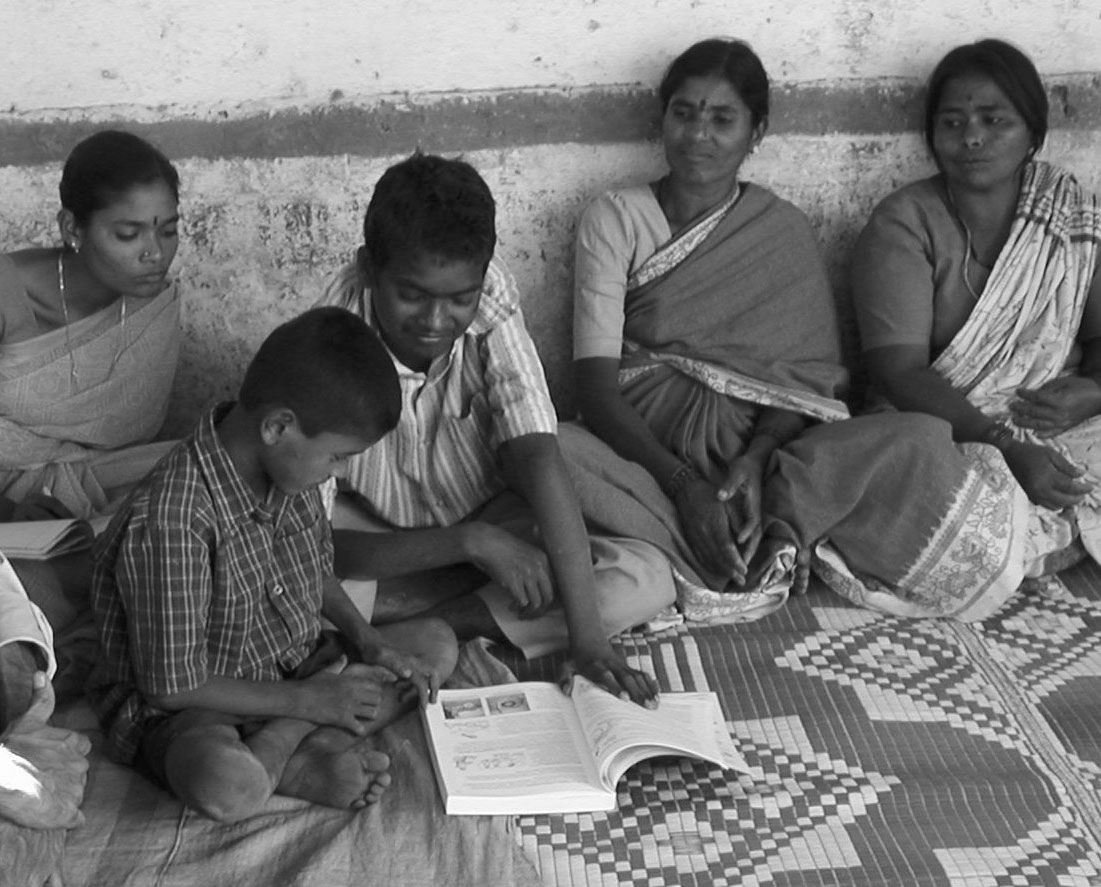
We told the group about the rustic “Playground for All Children” at PROJIMO in rural Mexico, and about the play and rehab equipment that the disabled children had made at the sangam in Gundmal. Pulling out a copy of Nothing About Us Without Us, I showed the sangam members drawings of easy-to-make playground equipment. The grown-ups showed polite interest. But the children were fascinated with the idea, and with the book. Two young boys poured over it for half an hour. One was Ram the angry retarded boy—who suddenly came to life. When the Sangam leader asked Ram if he would like to help build such a playground with other children, he scowled silently for a moment. Then with a big grin he nodded, Yes!
Integrating Disabled Kids Through ‘Child-to-Child’
One of the biggest benefits of schooling potentially, is that it gets children in a community working and playing together, as companions and even as equals. But this potential is not always met—and it is here that Child-to-Child can make a difference. Whether in school or out of school, it can help a group of children reach out, include, and assist “the child who is different.”
The Child-to-Child methodology started in the International Year of the Child (1979) and is now practiced in over 70 countries. It began with the idea of teaching school-aged children to help meet the health and development needs of their baby brothers and sisters. (For example, the importance of giving lots of fluid to an infant with diarrhea.) But Child-to-Child has evolved. Now it includes activities and games to sensitize children to relate in a friendly and enabling ways to children with special needs. (Our books Disabled Village Children and Nothing About Us Without Us both have sections on Child-to-Child disability-related activities. Both books are available in full on our web site (www.healthwrights.org)
In Gundmal, Hakeempet, and other sangams, whenever we discussed Child-to-Child, there was a lot of interest, especially among the children. I am happy to report that Commitments has followed up on this interest. In recent months, B. Venkatesh, who has a lot of experience with Child-to-Child, con-ducted Child-to-Child training workshops for prospective facilitators from different mandals. Fittingly, the first workshop was held in Gundmal, where the disabled children in the Aruna Sangam played a central role. Leadership by the children themselves is a key to success of Child-to-Child.
Possibility of Disability Sangams in Managing Community Based Rehabilitation
On our visits to the sangams, we encountered a strong felt need for Community Based Rehabilitation (CBR). Currently families have to travel far and spend lots for even the most basic rehabilitation services or assistive devices. To make things worse, private doctors and traditional healers often exploit poor families by prescribing medicines or herbal remedies for mental retardation, cerebral palsy, and other disabilities that require developmental rather than curative measures. (See photos, page 4)
Members of various disability sangams were eager to start a CBR program in their village. In our discussions , the idea arose that one or two sangam members could be trained as CBR workers, and the rest of the sangam could assist them. The necessary training and back-up, and referrals could be arranged by Commitments, SERC and the State government. The neighborhood houses could be used as a CBR center. Already the disabled youngsters in the Aruna Sangam, on their own initiative, were moving in this direction.
The leadership of Commitments and SERC was already thinking along similar lines. Disability sangams could become involved in CBR activities, first in selected villages where interest and potential were high. They might begin with informal peer counseling. (For example, a mother with years of experience assisting her disabled child could advise and assist less experienced mothers.) CBR training could be incremental. Through short workshops, trainees (chosen for their interest, ability and compassion) could be taught basic skills. Through hands-on apprenticeship, they master aspects of physical rehabilitation. They could employ Child-to-Child activities to help special needs children gain entry into schools. They could lead activities to promote community respect and opportunities. And they could organize prevention campaigns.
Development of CBR activities at the village level is one of the program goals. However, in the Mahabubnager project, rehabilitation services are still largely provided by visiting professionals. While a good back-up and referral system is essential for effective CBR, much more needs to be done to train local CBR workers at the village level. And if these CBR workers are disabled persons, their commitment, empathy and quality of work is likely to be better.
In some of the disability sangams, such as in Gundmal, there are bright young disabled persons who would jump at the chance to become village CBR workers, and would likely do an excellent job. Some might go on to become leaders for human rights in their communities. Their contribution would help win appreciation and respect for disabled persons in general.
(For examples of how this empowering process has evolved in Mexico and elsewhere, see the books, Disabled Village Children and Nothing About Us Without Us.)
Wanted: Village Health Care
In the villages the lack of adequate health services is a huge problem, especially for disabled people and the “poorest of the poor.” In theory, Primary Health Care in India is a universal human right. In practice, hundreds of millions of people face enormous obstacles to getting the health care they need.
In India government health services exist on several levels. At the village level are the “anganwadis” or village health workers, mostly village girls with a couple of weeks training. Their skills and responsibilities are so limited that they have little credibility among the villagers. They weigh babies, fill out forms, and help rally people for immunization. However, they are taught almost no curative skills. They know less about useful medicines (most of which they are forbidden to use) than do local shop keepers or the traditional healers. They refer the sick or injured to the closest District Health Center.
But District Health Centers (the second level of service) are few and far between. Time and cost to get there, and the series of bribes or “tips” required to get service, are such that the poor often go untreated. Or worse, they use up their limited food money on transport, bribes, and (recently introduced) “user fees” (or, alternatively, on local private doctors.) As a result, their hungry children become even less resistant to the “diseases of poverty.” Thus “health care” becomes another cause of ill health, disability, and death. Health department officials concede that the services of district health centers are often inaccessible to the most disadvantaged.
At the third level are public hospitals and surgical centers in larger towns and cities. Indigent and disabled persons are legally entitled to free care, along with “entitlements” such as bus and train passes. But again, the combination of bureaucracy and corruption (bribes) deprives the neediest people. Underlying these problems is the fact that the government budgets only a small fraction of what is needed to provide the services and entitlements guaranteed by law.
An Enormous Unmet Need: All this means that in rural Andhra Pradesh there is an enormous need for low-cost, competent, health services provided by, caring health workers at the village level.
A Possible Solution: Disabled Persons as Health Workers, Backed by their Sangams
In our discussions with villagers, SERC, and the APRPRP planners, an exciting possibility arose. Why not train selected members of the disability sangams as village health workers (VHWs)? A comprehensive, participatory approach to Primary Health Care could be revived at the village level. Young disabled women (and men?) from the sangams could be trained as an upgraded version of anganwadis. Their sangam could form a back-up team for health promotion. The new anganwadis (or VHWs) could embrace preventive, curative, rehabilitative, and promotive curative aspects of PHC in a manner that could more fully protect health of the poorest, most vulnerable people. Backed by their sangams, they could involve other (non-disabled) sangams, school children (through Child-to-Child activities) and other villagers, in health promoting action. Together they could address issues such as water supply, sanitation, malaria control, tree-planting, sustainable agriculture.
This way, disabled persons would play a central role in the community’s well being. People would look at their strengths, not their weaknesses, and include them more fully.
This approach could also help bring about closer links between Primary Health Care and Community Based Rehabilitation. The “Neighborhood Houses,” might evolve into Community Based Rehabilitation and Health Promotion Centers”—as part of an empowering village-based development paradigm.
Good Health Care Reduces Poverty
Studies in India show that on the average poor families spend 19% of their family income on health care-related expenses. Costs related to catastrophic illness are one of the main events that push families that have managed to cope into absolute poverty.
Empowering communities to better meet their health needs at low cost can be an important step toward reducing poverty. In the long run it can save more money than it costs (for people and government alike).
Potential for ‘Scaling Up’
Within the self-help disability sangams in Mahabubnagar, the interest and potential exist to improve health and rehabilitation services at the village level. Such an empowering approach could help meet an urgent need of the most vulnerable people. It would also increase respect and opportunities for disabled persons. And reduce poverty.
This community-based approach could be introduced, on trial basis, as part of the Andhra Pradesh Rural Poverty Reduction Program. The APRPRP, as a state-wide program, has the necessary links to government and to the health, education, and other relevant ministries. If successful, the approach can be incrementally scaled up to include all 500 mandals under the coverage of the APRPRP. And from there, who knows?
Conclusion
Clearly, to substantially reduce poverty in India—or anywhere else—will require trans-formation of unjust socioeconomic and political structures that go far beyond village-based health and rehabilitation measures. But in the meantime, such measures can help the most vulnerable villagers cope a bit more successfully. By coming together to solve their problems, perhaps in time a critical mass of “people who care for one another as equals” will be reached so that, collectively, they can begin to demand and work for more far-reaching change.
End Matter
I m p o r t a n t : We lost part of our current mailing list due to a computer glitch, and are trying to rebuild it. If there is any error in sending out this newsletter, or discrepency in number of issues due, please let us know. Thanks!
Please Note! If you prefer to receive future newsletters online, please e-mail us at: healthwrights@igc.org

| Board of Directors |
| Trude Bock |
| Roberto Fajardo |
| Emily Goldfarb |
| Barry Goldensohn |
| Bruce Hobson |
| Donald Laub |
| Eve Malo |
| Myra Polinger |
| Leopoldo Ribota |
| David Werner |
| Jason Weston |
| Efraín Zamora |
| International Advisory Board |
| Allison Akana — United States |
| Dwight Clark — Volunteers in Asia |
| David Sanders — South Africa |
| Mira Shiva — India |
| Michael Tan — Philippines |
| Pam Zinkin — England |
| María Zúniga — Nicaragua |
| This Issue Was Created By: |
| David Werner — Writing and Photos |
| Shefali Gupta — Technical Assistance |
| Trude Bock — Proofreading |
It is not a sign of good health to be well adjusted to a sick society.
— J. Krishnamurti (1895-1986)