



































































Nicaragua—Hands-on Workshops: Learning to Make Low-Cost Assistive Devices for Disabled Children
In May, 2005, The Association of Parents of Disabled Children, better known as “Los Pipitos,” invited David Werner to visit them in Nicaragua. Los Pipitos began in 1987 when a small group of parents in Managua came together to look for ways to meet their disabled children’s needs. But it has grown amazingly. Today Los Pipitos has over 60 chapters in towns throughout Nicaragua. In the early years most of the children had developmental delay, mainly Down syndrome. But today kids with all sorts of disabilities are welcome. Thousands of families are involved.
‘Security Measures’ an Obstacle to Exchange Visits
My invitation to Nicaragua grew out of a frustrated attempt by three physiotherapists from Los Pipitos to visit PROJIMO in Mexico in 2004. For years the books that grew out of PROJIMO (Disabled Village Children and Nothing About Us Without Us) have been valued sources of ideas and innovation for both families and therapists. These books have proved especially useful now that Los Pipitos has begun a Community Based Rehabilitation (CBR) initiative, as it tries to extend into rural areas and marginalized communities.
Unfortunately, the Mexican Embassy in Managua refused to grant visas to the physiotherapists from Nicaragua. Even when HealthWrights contacted the Mexican Ambassador, explaining the humanitarian purpose for the visit, the visas were “regretfully denied for security reasons.” Evidently this new restrictive policy by Mexican immigration is due to pressure from the US government. Since 9/11 it fears that Central Americans, even employed professionals, will use Mexico as a bridge for illegal entry into El Norte. So in lieu of visiting PROJIMO, Los Pipitos invited me to visit them. Likewise present at the seminar, and participating in the subsequent workshops, were more than 20 “mediators” from Stichting Liliane Fonds (SLF), a Dutch Foundation that provides assistance to needy disabled children throughout the developing world. Many of these SLF mediators are also active leaders in Los Pipitos. SLF has been enormously helpful to PROJIMO in Mexico.
The Managua Seminar
During my week in Nicaragua, the organizers of my visit set up an intensive but exciting agenda. First was a full day “encuentro” or seminar in Managua titled “Assistive Measures, Independent Living, and Community Based Rehabilitation.” The 250 attendees included representatives of Los Pipitos from all over the country, staff from the Health Ministry, and key persons from the universities and various charitable organizations.
Likewise present at the seminar, and participating in the subsequent workshops, were more than 20 “mediators” from Stichting Liliane Fonds (SLF), a Dutch Foundation that provides assistance to needy disabled children throughout the developing world. Many of these SLF mediators are also active leaders in Los Pipitos. SLF has been enormously helpful to PROJIMO in Mexico. The whole day of the seminar was devoted almost completely to my presentations. Using PowerPoint pictorial graphics (mostly photos and drawings), I gave a series of presentations including:
-
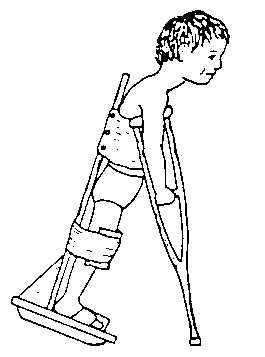
Crutches for Pipi—a story showing the importance of learning from one another and problem-solving as equals (adapted from Disabled Village Children)
-
Overview of PROJIMO—how it differs from the standard CBR approach.
-
Community Based Rehab (CBR) and the Independent Living Movement—the challenge of combining the best and avoiding the weaknesses of both.
-
Child-to-Child activities—a discovery-based approach with a focus on inclusion of disabled children.
-
Four Women in Four Lands—the importance of adapting assistive devices to the local environment.
-
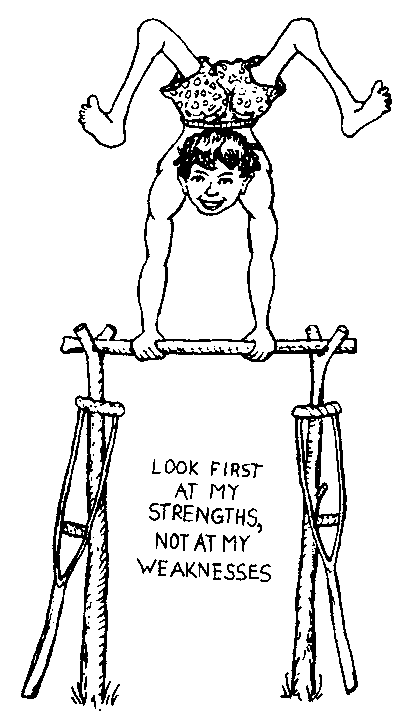
True stories that graphically illustrate key principles such as, “Look at my strengths not my weaknesses,” “Liberation, not normalization!” “Making therapy functional and fun,” and “Nothing About Us Without Us.”
LOOK AT MY STRENGTHS, NOT MY WEAKNESSES
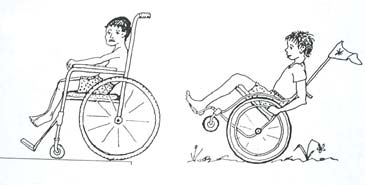
In the Managua Seminar, David told “The Story of Jesus” to demonstrate the disabled persons’ motto: “LOOK AT MY STRENGTHS, NOT MY WEAKNESSES.” The narrative concerns Jesus Orosco, a Mexican boy with spina bifida who lost one leg due to bone infection and then became visually impaired. Jesus came from a very difficult home situation. But with help from PROJIMO and Child-to-Child activities, as he has grown up he has become a very caring, hard working rehabilitation worker—and wheelchair racer in a three-wheeler he helped build. Jesus has developed incredible strength in his arms and upper body.
|
|
|
Everybody has a Story
With such a large audience, in the seminar it was not easy to get everyone participating. But some interaction was achieved through story telling. After telling an eye-opening true story I would ask people to tell a similar story from their own experience. For example, following my story of “Crutches for Pipi,” participants gave their own examples that show how, when professionals and family members learn from each other and draw on each other’s skills, the results are often better. (The same is, of course, true when the speaker at a seminar draws on the knowledge of participants.)
Hands-on Workshops
The seminar on May 23 was followed by two regional “learning by doing” workshops in which participants had the experience of making simple assistive equipment for disabled children. Two rehab workers from Los Pipitos had taken part in a similar workshop I had facilitated in Medellin, Colombia, in 2004 and had been eager that I conduct such workshops in Nicaragua.
To allow broader attendance, the two workshops were held at opposite ends of the country. The first was held in Jinotepe, to the south of Managua. The second took place in Condega, near Estelí, close to the Honduran border. Each workshop was conducted in a learning center for disabled children run by the local branch of Los Pipitos.
Guiding Principles
The process is as important as the product. These short (2-day) workshops have 3 pragmatic learning-by-doing objectives:
-
Demystification: We can do it ourselves! Theworkshop provides an opportunity for persons involved in the care and rehabilitation of disabled children to have hands-on experience, first in evaluating the needs and wishes of the child and family, and then in designing and constructing simple, low-cost aids, using local materials.
-
Inclusion: We can do it together! The child and family must be included in the problem-solving process. The workshop encourages close partnership, or collaboration, between providers and recipients. Professionals and rehab workers work together with family members and the child herself or himself in determining needs and possibilities, and in planning, designing and creating appropriate assistive equipment.
-
Flexibility: We can adapt! By first visiting the child’s home, observing the living situation, and exploring needs and possibilities with the child and family, all learn that assistive equipment must be adapted to the specific needs of the child and the local environment.
Small is Beautiful
It is best that each workshop have at most 30 participants. More makes full participation difficult. But, as it happens, usually far more persons show up. In Jinotepe there were more than 50 participants, and in Condega more than 70, counting the disabled children and their family members involved.
|
|
|
|
|
|
Guidelines for Conducting a 2-day Device-Making Workshop
To follow is an outline for the type of two-day learning-by-doing workshop that I (David Werner) have facilitated in Nicaragua and many other countries. I provide this outline for two reasons. First, organizations that ask me to conduct such workshops in the future can use it to prepare appropriately. Second, I hope some programs can use these guidelines for planning their own workshops, without need of my presence. (The goal of any leader or facilitator should be to make oneself unnecessary as quickly as possible.) In brief, the 2 days of the workshop are planned as follows:
The first day starts off by learning about principles and approaches to making low-cost aids adapted to a disabled child’s specific needs, and then involves small group visits to the homes of pre-selected disabled children to evaluate their possibilities and plan for making an appropriate aid.
The second day involves collectively making the aids, in small groups, for and with the children and their families. It ends with demonstration of their use, and evaluation.
Outline of the Workshop Activities
Day 1: Preparation, Methodology, and Home Visits
Morning: Preparations
-
Discussion of procedure & goals for the 2 day workshop (1/2 hr.)
-
Presentation methods for evaluating the needs and possibilities of specific disabled children, and for making appropriate assistive devices (2 hours, with use of PowerPoint slides)
-
Preparation for afternoon visits (1/2 hour):
-
Participants divide into small groups, each with 4 to 5 persons.
-
Each group is given a copy of Disabled Village Children and Nothing About Us Without Us, and perhaps other resources. Ideally these can be distributed in advance.
-
Each group needs to have:
-
paper for taking notes and making drawings
-
pencils with erasers (for preliminary sketches)
-
measuring tape
-
poster paper
-
-
Transportation and procedures explained for home visits
-
Lunch (maximum 1 hour - or less to allow more time for visits)
Afternoon: Home Visits
-
Travel time & home visit: about 2 hours.
-
Each small group will travel to the home of a disabled child.
-
Important considerations in preparing for the home visits:
-
These visits must be carefully arranged in advance, choosing families and with children who are likely to respond well to a group of concerned strangers.
-
A family member must be willing to spend the whole next day participating in the hands-on workshop.
-
The visits should be to homes of poor families with disabled children with significant unmet needs.
-
The different children selected should have a range of different disabilities needing different simple assistive devices (ones that can be made in a single day).
-
Some children selected should be mentally alert and able to express their wishes, and if possible, to participate actively in building their own assistive device.
-
During the home visit participants, together with family members and the child herself, explore the child’s needs and possibilities. The child should be central to this process. Every effort should be made to gain the child’s confidence and listen respectfully to her desires. Even children who can’t speak often have ways to communicate their likes and dislikes, and these should be heeded. The families’ concerns, wishes, and ideas should also be central to the process.
-
The learning group (including family and child) considers possibilities for an assistive device that might help the child do something she wants, or that helps the family better manage the child.
-
To get ideas for possible aids and designs, the participants can look in their books and show pictures to the parents and the child.
-
When a likely aid—or combination of aids—is mutually decided upon, the group draws sketches and takes measurements.
-
When one or more aids are decided upon and sketches drawn, the group copies the drawing on poster paper for next day presentation.
-
Before leaving, the group makes sure the child and at least one family member agree to attend the day-long workshop the following day, and that arrangements for transportation are firmed up.
Day 2: The Workshop: Making Assistive Equipment For and With Each Child
-
The workshop, if possible, is held in a community rehab center, carpentry shop, or other facility where assistive equipment is made or repaired. (A community shop run by disabled persons is ideal.)
-
The workshop is attended by up to 30 enrolled participants, plus each of the disabled children with a family member who were visited the day before. The family member and child are urged to be participating members of each group, with full involvement of planning, building, and evaluating the aids.
-
Because workshops last all day (up to 8 hours), provisions must be made for children to play, eat and nap—as well as participate.
Timetable for the 2nd Day (the Device-Building Day)
Opening plenary. (1-1 1⁄2 hours) Each group presents the evaluation of the child’s needs, wishes, and possibilities, and displays the poster with the designs for one or more assistive devices. All participants including family members and children are invited to make suggestions.
-
Small group activity. Production of the aids (5-6 hours)
-
Final plenary. Presentation and evaluation (1 hour) Each group presents the aid or aids it has made, and the child and family member demonstrate how they use it. The audience makes constructive observations and applauds the successes (or at least the efforts).
-
Closure and congratulations (15 minutes)
-
Be sure follow up is planned for devices that still need work.
Cautions and Advice for Making Aids
Before beginning the construction of the devices, participants should be precautioned:
-
When making an assistive device, first put it together in provisional form, so you can test it with the child and make needed changes. Use screws. Or if you use nails, leave the heads out a bit so you can pull them out easily to make changes. Don’t use glue until you’re sure everything is just right.
-
Don’t paint or upholster the aid until after it has been well tested by the child and everything appears to work well (often several days of trial are needed). In the workshop it is better to give more time to getting the aid to function just right. Making it pretty may also be important but can come later.
-
In making the aid, try to pace the work so that construction is completed in plenty of time to allow for repeated testing and modifications.
-
Try to divide up the tasks so that everyone in the group, including the family member and, as much as possible, the child, keep active.
Plans for Follow-up
It is important that follow-up is arranged to assure the completion of any aids that are still incomplete or need rework or modification. Every effort should be made that the assistive device actually serves its purpose and the child and family like it. Follow-up is essential.
Successes and Challenges of the Nicaragua Workshops
Nearly everyone agreed that the workshops were a great success. The final, pragmatic measure of success is if the aids helped the children do things better, and many did.
This is not to say that all the assistive devices turned out well. Some of them worked remarkably well. Others were more or less OK but needed improvements. And a few had major problems. But people can learn as much or more from their mistakes as their successes. Indeed, at the start of the workshop it was pointed out that to make assistive equipment for a specific child is often a process of trial and error. We shouldn’t expect that everything will turn out just right the first time. Even when something turns out well, there is always room for improvement.
An indisputable achievement of the Pipitos workshops was the enthusiasm, hard work, and full involvement of all the participants. One goal of the workshop was to get rehab workers, family members and the disabled children themselves working together, both in sharing of ideas, and in production of the aids. To a large extent, this happened. It was wonderful to see all the interaction and cooperation. Mothers of the disabled children pitched in eagerly. And two of the fathers, experienced in working with wood and making things, took the lead in creating the aids for their own children, as well as generously assisting other groups.
The active participation of disabled helpers and local crafts-persons was, to me, one of the delightful features of the workshops. In Jinotepe, where the Pipitos Learning Center has a carpentry shop, three mentally handicapped young apprentice carpenters helped our workshop participants who were making assistive devices with wood. Since there were no electric cutting or sanding tools, everything had to be done by hand, and this slowed down work a lot. Fortunately, the disabled young men had incredible stamina and good will, especially on that blistering tropical day. Without their enthusiastic help, some assistive devices would never have been completed.
On the afternoon of the first day, one of the young mentally handicapped carpentry apprentices who was most helpful had an epileptic seizure. For several minutes he lay twitching on the floor, while people gently protected him from injuring himself. However, the next day in the workshop the same lad was working away at full tilt. So everyone looked at his strengths, not his weaknesses.
|
|
|
On our way to Condega, we visited the “Centro Juvenil” in Estelí, a huge new complex of spacious buildings for the skills training of disabled youth, financed by the European Union and others. There, we met Melvin, an 11 year old boy with muscular dystrophy. Melvin’s big wheelchair had no footrests.
Because footrests are important for comfort and to prevent foot-drop contractures, we invited Melvin to the workshop the next day, where he could help make his footrests. A local carpentry instructor offered to take him, and was good to his word. In the workshop he and a carpenter with polio pitched in enthusiastically wherever they were needed (see below).
Remarkable Creativity and Productivity: What We Made
I have facilitated assistive device workshops in many countries and circumstances, but rarely have I encountered participants as enthusiastically productive and creative as in these workshops with Los Pipitos. In the two days of constructing the aids, the participants produced nearly 50 different assistive devices, ranging from very basic to very ingenious.
Examples of aids made included:
-
Special seats, some made of wood, some of plywood, and some completely or partly of laminated cardboard (paper-based technology)
-
Standing frames, of wood, of laminated cardboard, and combined materials
-
Modified seating for better positioning and function in wheelchairs and other chairs
-
Adaptations to give a child better mobility in his outrageously oversized wheelchair
-
Tables for chairs and wheelchairs Modification of wheels on a commercial walker to improve balance
-
Wooden commode stool for easier, happier toileting
-
Leg splints to allow a diplegic child to start walking
-
Enclosed wooden swing
-
Toys and rattles for manual dexterity and early stimulation
-
Hanging mobiles for eye use, head control, and developing use of hands
-
Reclining cardboard wheelchair insert
-
Special bed for sleeping and for learning to walk (holding onto it)
-
Torsion cables to correct foot position and improve gait
-
Head-pointer for writing (for a girl with arthrogryposis and no hand function)
-
Adjustable stand for mouth-writing, which adjusts into a tray for independent eating
-
Cardboard arch supports to correct foot deformity
-
Parallel bars made of rope to improve balance
-
Night splints (padded plaster of Paris) for improving position of feet
-
Footrest for a wheelchair for comfort and to prevent contractures
|
|
|
|
|
|
|
|
|
|
Innovation: Torsion Cables to Straighten Christopher’s Feet
One of the most original aids constructed at the Condega workshop was made for Christopher, a bright 8-year-old boy with spina bifida. To help him begin to walk, Christopher had previously been fitted with plastic below-the-knee braces (AFOs).
When the boy’s group visited his home, they asked him what he most wished he could do. He said “Caminar mejor!” (Walk better).
Christopher ’s gait was very wobbly and unstable. His feet pointed out to either side rather than forward. Other kids teased him. On examining the boy, the group found he had dislocated hips, and very little muscle control for rotation of his legs. A physiotherapist in the group thought that making parallel bars for him to practice walking might improve his gait. But for Christopher—who could already walk, if poorly, without holding onto anything—this seemed like a big step backwards. What to do? On looking in Nothing About Us Without Us, the group found illustrations of “torsion cables”—flexible hoses that run from the waist to the shoes. They are twisted so as to rotate the angle of the feet into better position. They are often used for a child whose feet turn inward (pigeon-toed). But why not for a child whose feet rotate outwardly. No one in the group had experience with such cables, or was sure that if they managed to make them they would work. But the family was eager and I encouraged the group to try. Christopher’s father fetched a thin-gauge plastic garden hose (about 1.5 cm diameter) from the patio. They tried twisting it to see how much torsion it could provide, and it appeared to be enough.
The next day both Christopher’s parents went to the workshop with their son, and and worked closely with their group. They started explaining their plans, showing their design to everyone. Then they started making the cables.
|
|
|
Someone bought a leather belt in the market. To this they attached the top ends of the hoses with nuts and bolts. Rather than attaching the bottom end of the hoses to the heel of the shoes, which is the usual way, they bolted the hose to the outer side of the boy’s plastic braces. When completed, to put them on, they twisted the hoses outwardly enough so that they would in turn gently rotate his feet inwardly. To everyone’s delight, when Christopher tried walking with his new “hoses,” his feet pointed in a much more forward position, and his gait improved conspicuously.
Another innovation was to conceal the torsion hoses from view. Typically such cables are worn outside the pants. This can make the child look “weird” to other children: “He looks like a Martian!” So the group decided to fit the hoses inside his pants. Both the boy and his parents applauded the idea.
A foot wedge to correct foot deformity. An additional problem with Christopher was that one foot was developing a contracture that bent it inward and downward (equino-varus). Even inside the AFO, the foot bent over when he walked. This further compromised his gait. To help correct the problem, the group made a simple laminated cardboard insert to put inside the brace, so that when he walked it would help stretch and correct the deformity rather than worsen it. Impressively, with the insert, Christopher dipped less to the side and his gait improved.
In the final evaluations, when Christopher showed everyone how much better he could walk, all were amazed. The suggestion was made that a stronger hose could give a bit more torsion, to rotate Christopher’s feet even a bit forward. I pointed out that in PROJIMO they use hoses for gas welding to make torsion cables that provide a stronger, more resilient twist. Christopher’s father, who had played a key role in making his son’s device, said he would get some gas welding hose and make them himself. He knew what to do because he’d taken part.
All in all, Christopher’s success was a wonderful example of how simple innovative aids can be made by working closely with the child and family—and how, by including the family in the problem-solving and creative process, the family becomes empowered to take the lead themselves. Family empowerment of this sort can in turn lead to long term benefits for the child, the family, and the whole community.
Paper-based Technology
One of the most promising technologies practiced in aids-making workshops is the use of laminated cardboard, made by gluing together the walls of corrugated cardboard cartons. Although some of the Los Pipitos participants had read about “paper-based technology” in Nothing About Us Without Us, only one person had actually used it.
But many were eager to try it. The building materials—old cardboard cartons—are cheap, easy to work with, and amazingly strong when carefully laminated with homemade flour paste, or (for faster drying) white glue. Yet the finished aid has enough softness and “give” that it lends itself to many kinds of children’s assitive equipment.
Note: It is important, several days in advance of the workshop, that large, sturdy cardboard cartons be collected, laminated in large squares, and pressed flat until thoroughly dry. If the cardboard is laminated the same day the aids are made, it will still be damp and flimsy. (For instructions see Nothing About Us Without Us, page 72.)
In Los Pipitos workshops, participating groups used laminated cardboard for several kinds of aids, including those shown here:
|
|
|
|
|
|
There are many more examples of paper-based technology in this newsletter. Groups sometimes used cardboard in combination with wood and other materials. They used it for foot separators on parapodia, protective cushions, seat backs, and wedges for better posture. But the most frequent use was for special seating.
|
|
|
A Table and a Swing for Yelvin
Visiting the children in their homes proved important for making aids to match their needs. Yelvin is a stunted, developmentally delayed nine-year-old boy. He lacks balance but can take wobbly steps when held upright by his hands. Had the group not visited his home, they might have recommended a wheelchair or walker. But visiting his home made clear such aids would be of little use there. His family lives in a tiny pole-wall shack in the forest at the end of a steep trail.
There is no furniture in the hut except for a small wooden chair that Los Pipitos made for Yelvin. A rough wooden plank on posts is the only semblance of a bench or table. The family stands or sits on the ground to eat. The terrain outside is too rough and steep for a wheelchair, and even inside is too uneven for most walkers.
In the home the group experimented by stretching two ropes as improvised parallel bars. With a bit of encouragement, Yelvin held the ropes and gingerly took a few steps, trying to get his balance.
This seemed better than firm wooden bars because it seemed to help him gain more balance and advance toward walking alone.
Among the most promising resources in the hut was a gaggle of young boys from a house higher up the slope. The boys were eager to help, and we showed them how they could have Yelvin hold a rope stretched between their hands, encouraging him to take steps. This requires more balance than simply holding onto his hands.
All considered, what the family seemed to want most was a table where Yelvin could eat. So the device the group decided to make was a table that could attach to his chair, which they also repaired. In addition they built a rack over the table from which they could hang toys to stimulate the use of his hands.
However the aid that Yelvin enjoyed most was an enclosed rope swing, made ingeniously with bars of wood with holes that the rope passes through. Yelvin’s grand smile was the measure of success.
Helping Karla Draw, Read and Write, and Drink
Karla is a 23 year old girl born with joint deformities (arthrogryposis). She rarely leaves home and cannot read or write or feed herself. But wants to. She has a wheelchair but greatly prefers her rocking chair.
Holding a pencil in her mouth, she was able to draw if someone held paper for her. Karla’s group started by helping position her more comfortably in her rocker. (See the photos in Paper-based Technology, below).
So for the time being she prefers using her mouth. Los Pipitos is going to find a way to help Karla learn to read and write. I (DW) have put her in touch with a world-wide club of persons with arthrogryposis.
The Biggest Successes—Two Poster Children Who Walked for the First Time
Surprisingly, the two children for whom aids built in the workshops perhaps made the biggest difference both happened to be “poster children” for the national Telethon.
Ironically, both these “child symbols” for El Teletón are also symbolic of the large number of children who have received assistance and equipment that is inappropriate for them, or even counterproductive in terms of helping them reach their potential.
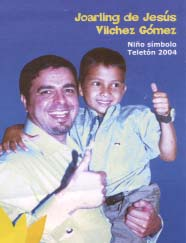
Joarling
Joarling, the Teletón 2005 poster child, is a bright 8-year-old with spina bifida. To help him get around better, he was given a magnificent hand-powered tricycle.
Joarling loves his trike. But when participants visited his home, he confided that his biggest wish was to walk. With adequate bracing and crutches, clearly he had walking potential; he could lift his full weight with his arms, and had minimal contractures in his hips and knees. Yet for all these positive signs, rehab professionals had made little effort to get him walking. Perhaps they had been taught that: “Spina bifidas don’t walk.”
Responding to the boy’s wishes, the group decided to start Joarling off with a standing frame. But considering his arm strength and high motivation, I guessed he might be able to begin walking with a parapodium (a kind of standing frame designed for walking), first on parallel bars, later with crutches.
No one had ever seen a parapodium, much less made one. But on looking at the pictures in Nothing About Us Without Us, everyone wanted to give it a try, especially Joarling.
When his parapodium was done and they strapped the boy into it, he found he could stand securely upright without holding on to anything! Then, standing between the parallel bars, to everyone’s amazement he at once fearlessly began taking big steps, swing-through easily between the bars. He laughed with joy and everyone applauded. Joarling loved his parapodium.
Joarling walked so well on the bars that he wanted to try crutches. Although only an hour remained, the two volunteer carpenters, one a crutch-user himself, quickly made a splendid pair of adjustable crutches.
When the crutches were finished, Joarling tried them. They still needed adjustment, and he needed practice. But it was clear he would soon be bounding about on them. In the following weeks he scampered all over town. We warned him to start cautiously, and check his feet often for sores, since they lack feeling.
Evert
Evert, the other Teletón poster child, is a five year old boy with diplegic cerebral palsy. Like Joarling, he too had a potential for walking. Perhaps because of the spastic scissorng of his legs and weak thighs, no one had tried leg supports to see if he could walk. But Evert had good strength and control in his trunk and arms—and was eager.
Evert’s group made two padded wooden splints, which they strapped to the backs of his legs to keep his knees straight. With these he was able to stand between the parallel bars.
Valiantly Evert made an effort to take steps, but his legs scissored too much. However, when a foam roll was placed between his thighs, it separated his legs enough that he could actually take steps. Soon he was walking back and forth between the bars smiling happily.
The group had at first thought to make a standing frame for Evert—but then decided on a parapodium, to walk with. To discuss the relative merits of each, they made cardboard models.
The parapodium they built had some problems (nails too small). But with reinforcement it was clear the boy could learn to walk with it.
Obviously, both Evert and Joarling have great potential for walking. The improvised aids are a good start. But to meet their full potential, they will need good orthopedic appliances. However, obtaining such appliances in Nicaragua is often not easy. (See below.)
The Paradox of Professional Expertise
One perplexing observation that I and others observed in the Pipitos workshops was that often the most effective rehabilitation aids were created, not by the rehab professionals, but by caring lay persons.
Most of the active members of Los Pipitos are parents—mainly mothers—of disabled children: volunteers with a lot of empathy who reach out to help families and children with similar needs. These parents comprised the majority of the workshop participants. The assistive devices created by these dedicated lay workers often came closer to meeting the specific needs of the children than did those spearheaded by the more highly trained professionals.
One reason for this paradox, I think, is that the lay persons were less sure of what was needed. Therefore they took a more exploratory, open-ended approach. They were more willing to listen to the ideas and wishes of the child and her family. And they were more inclined to look for ideas in their books, to discuss the pros and cons of different aids for the child in question, and to use those designs in the guide books not as something carved in stone but as a springboard for designing a device adapted to the unique needs of the child. They were guided not by preconceptions, but by love.
By contrast—with several refreshing exceptions—the professionals tended to think in a box and to prescribe by rote. If the child had such-and-such disability, he could achieve this, but not that. According to the label she was tagged with, she needed this kind of assistive equipment and not that. As a result, the assistive devices that the professionals designed for a child tended to be generic, not individualized. They were skillfully constructed and beautifully decorated, yet often didn’t quite match up with the needs or wishes of the child. Too often they tried to adapt the child to the device rather than the device to the child.
For example, when the professionals took charge of producing a special seat for a child, it was often box-like and visibly uncomfortable. Everything was squared off, stiff, and non-adjustable. The back was straight up and down. Worse still, the finished seat often didn’t fit the child. Yet the errors were hard to correct. The experts were so sure they were right, they would nail and glue it together with finality, or paint and upholster it, before adequately testing it with the child. As a result, in the final evaluation session when each device was demonstrated with the child using it, there were several occasions when devices conceived by professionals simply didn’t work.
One example was a very box-like seat made of laminated cardboard. Overall, the seat was too small for the child and did not provide adequate support. Yet at the same time the seat was so high that the girl’s feet dangled several inches above the floor. To correct the error, my books came in handy—as a footrest! But if the books had been used earlier for planning and problem-solving, the results might have been more functional.
Volunteer carpenters outstanding In Condega, two of the most capable and innovative participants in the workshop were two local carpenters. One had a disability from polio. The other taught in the “Centro Juvenil” in Estelí (see page 4).
In the workshop the two local carpenters pitched in enthusiastically, with both creativity and skill. One of their most remarkable feats was their rush job of making adjustable wooden crutches for Joarling.
An Aid That Wasn’t
Another example of an aid that backfired, overseen by a very caring physiotherapist, was a standing frame for Marlon, a child with spastic cerebral palsy.
The group did a fine job making the device out of laminated cardboard. However everyone was so sure it would work well that they upholstered it beautifully with vinyl before testing it. Indeed, this took so long that they were late for the final plenary evaluation. Then, when the boy finally tried it, it proved to be less of an assistive device than an instrument of torture.
Errors included:
-
Wrong measurements. Frame should reach chest but reaches chin.
-
Top of frame is too wide. Child can’t reach forward to play while standing.
-
Misplaced vertical struts. When the boy’s feet are placed through the footholes in the frame, his toes jam into the struts. Ouch!
-
Painful foot-lifts. Beneath each foothole was a thin bar under the fore-foot to stretch heel cords. However, the foot-holes are too small for shoes, so he has to stand barefoot, his whole weight on the 1⁄2 inch wide bar pressing the bottoms of his feet.
Ouch, in every sense! But hard to change. It’s already upholstered.
Costly Imported Wheelchairs Are Not the Best Answer
Socio-economically, Los Pipitos is in a strangely polarized circumstance. On the one hand, in Nicaragua poverty is rife. Thanks in part to US covert and overt intervention over the last two decades, Nicaragua has now become the second poorest country in the Americas. (Haiti remains the poorest.) On the other hand, Los Pipitos, as the country’s largest and most successful program for dis- abled children, receives handsome donations from foreign charitable organizations, especially in kind. Additionally, the Teletón—the nation’s celebrity-driven event to raise money to help disabled kids—has helped Los Pipitos build spacious, impressively equipped rehabilitation centers in several cities (the edifice complex).
Yet for all this benevolent assistance, some big gaps remain in meeting children’s needs. One problem is that the fancy donated rehab equipment is not always well suited either for the children or the situation they live in.
Children’s wheelchairs are a case in point. I saw some children in wheelchairs that fitted them well. However for more than half the children, their wheelchairs were far too big or otherwise ill-suited. This limited rather than increased their function, and caused discomfort, poor posture, and increased deformity.
Fortunately, a team of Canadian seating specialists had helped adapt the giant wheelchairs by adding cushions, wedges, footrest lifts, etc. Yet these additions made the chairs even heavier and harder to move.
Improving Oscar’s Mobility
Oscar is a five-year-old who attends the Pipitos’ special school in Jinotepe. He has a huge bright red wheelchair with arm rests up to his shoulders. Oscar could only reach one wheel at a time. By leaning first to one side or the other, he could barely move the chair by contorting sideways to push first one wheel, and then the other. He depended on others to move.
|
|
|
Oscar’s group decided the only real answer was to get a wheelchair closer to his size. This would be a challenge for the future. Provisionally, however, they simply removed the armrests from his wheelchair. This allowed him to reach both wheels at once. (Removing the armrests wasn’t that easy; they were screwed hard into place.)
For a selection of individually designed wheelchairs made by PROJIMO in Durangito, see: www.healthwrights.org/sillas.
However, without the armrests the boy—who has spina bifida and weak pelvic control—felt unstable. So the group added a seatbelt, and the boy then felt secure. However at first the belt was attached too high and caused a bad position. Oops! So they repositioned the belt low across his lap. This helped him to sit in a better position. Now Oscar could propel himself well using both hands at once. He was overjoyed!
|
|
|
Why does Nicaragua have such a hard time finding wheelchairs that meet children’s needs? 25 years ago the Organization of Disabled Revolutionaries (ORD) began building low-cost, all-terrain wheelchairs. Today several shops, mostly run by wheelchair users, make and repair wheelchairs. Still, there are almost none for children.
Possibilities were discussed for ways to respond to this unmet need. We have approached Ralf Hotchkiss, founder of Whirlwind Wheelchair International (WWI) in San Francisco, to see if he can do something. He has long been involved with wheelchair-building programs in Nicaragua.
Another possibility we are exploring is for the PROJIMO wheelchair-making team in Mexico to train disabled Nicaraguans in designing and building children’s wheelchairs, as it has done for apprentices from several states in Mexico and Guatemala.
The Need for Low-cost Shops to Make Leg Braces and Other Assistive Equipment
Appropriate children’s wheelchairs are not the only assistive equipment hard to get in Nicaragua. There is great need for other ostensibly “high tech” aids like orthopedic appliances (braces).
Obviously, Evert and Joarling—the two poster children described earlier—both had a great unmet potential for walking. The walking aids improvised at our Los Pipitos workshop got them off to a good start. But to meet their full ambulatory potential, they will need good quality braces.
But in Nicaragua, such orthopedic appliances are hard to obtain. Made only in a few shops, they are outrageously expensive. Los Pipitos could benefit greatly by setting up a few easily accessible, low-cost brace shops, preferably run by disabled technicians.
As with wheelchairs, we (Los Pipitos and PROJIMO) are exploring the possibility of having a few disabled persons from Nicaragua apprentice brace making at PROJIMO in Mexico. Then Los Pipitos can set up an orthotics shop in Nicaragua, and then teach others—a kind of multiplying effect. We are working to overcome immigration obstacles. If anyone has suggestions, please let us know.
Conclusion and Suggestions
Overall, both aids-making workshops held with Los Pipitos in Nicaragua were judged a great success by all concerned: participants, families, and the disabled children involved.
As predicted, some of the assistive devices turned out better than others. When the time was up, some still needed work, and many called for follow-up.
But we all learned a lot through our mistakes as much as our successes. Above all the participants realized how important it is to include the families and as much as possible, the children themselves, in the problem-solving process.
Suggestions for Improvement
1. Allow More Time
Looking back at the experience, a suggestion was made by the organizers that the time scheduled for such an intensive, hands-on activity be extended from 2 days to 2 1⁄2 or 3 days (not counting the initial seminar). This would allow participants more time to finish constructing the assistive devices and test them more systematically. Another advantage would be that the final session—demonstration and evaluation—could be postponed to the next morning when everyone is fresh. That way, more time and energy could be devoted to critical analysis, thus adding invaluably to the learning experience.
A disadvantage, however, would be arranging for the disabled children and family members to either stay overnight or to travel to and from their homes an additional time (some families live quite far away). It is, of course, essential that the children and their family members be involved in evaluating the functionality of the aids produced.
2. More Emphasis on Sharing of Ideas, and of Learning Through a Problem Solving-Process
I returned from Nicaragua quite exhilarated. A great deal is being accomplished to benefit disabled children, and both Los Pipitos and the Telethon are make an enormous difference. Yet at the same time, much remains to be done.
Many disabled children’s needs are not adequately met, despite substantial input of resources and concern. One reason for this is that too that often persons with formal training in the field of rehabilitation, for all their good will, do not take a sufficiently observant, innovative, open-ended approach. Rather they tend to follow a routine, according to generic diagnoses and text-book expectations. Too often they do not adequately and humbly explore with the family and child, the child’s possibilities as a person in her or his own right.
There are, of course, outstanding exceptions: therapists who dare to climb out of the box to take a more personalized, creative, and empowering approach. It is important that parent cooperatives like Los Pipitos learn to hunt out and make the best use of these more liberated and liberating professionals.
3. Change Needed in Schooling—and in Selecting Who Qualifies
In terms of long term goals, it appears the overall approach to education needs to be changed. From primary school through professional training, a more open-ended, egalitarian, discovery-based approach is needed.
Also it would help if students going into the “helping professions” were selected less by grade point average and more by their creativity and open-ended humility. They need to be willing to work with other people, especially marginalized persons, as equals.
4. More Disabled Rehab Professionals and Technicians
Many women’s rights advocates think that more gynecologists and obstetricians should be women. By the same token, perhaps more physiotherapists and rehabilitation specialists should be persons with disabilities—or at least be close family members of disabled persons. Such family involvement is the intrinsic strength of Los Pipitos, as of other endeavors led by parents.
But parents alone are not enough. (Too often parents are overprotective.) Disabled children need caring role models who have similar disabilities.
This is why, when I facilitate an aids-making workshop, I generally insist that at least half the participants should be disabled persons. By insisting on half, in the final countdown usually at least 10% have disabilities. Often these disabled persons take the lead in creative problem-solving and are especially sensitive to both the felt and real needs of the disabled child. They are more ready to step outside the box and look at the disabled children’s dreams and strengths before their weaknesses and fears.
5. The Future of Los Pipitos: More Leadership by the Disabled Children as They Grow Up—and Scholarships to Prepare Them
For the above reasons, I hope that in the near future more leadership of Los Pipitos will be taken over by disabled children themselves, as they grow up. In some of the chapters of Los Pipitos this is already happening. Three cheers!
It would also be grand if Los Pipitos could provide scholarships and encourage some of their disabled young people to study in disability-related professions such as physiotherapy, occupational therapy, brace and limb making, wheelchair design, special education, audiology, human rights advocacy, and social transformation.
With more disabled persons in the rehab profession, perhaps our institutions would stop teaching by rote and putting nonconformists into suffocating little compartments.
Perhaps together we can begin to build a saner, kinder world that celebrates diversity and gives even the odd-balls a fair chance.
Appendix—to the Outline for an Aids-making Workshop: Tools and Materials
NOTE: The types of tools and variety of materials for the workshop can vary with the conditions. In poorer communities, you can use very low cost or scrap materials, including old cardboard cartons, or even mud. In communities with a few more resources, somewhat more costly items such as plywood and Velcro can make construction of assistive equipment easier, faster, and possibly more functional.
By the same token, depending on the situation, tools used can be more basic or more elaborate. Most aids can be made with only simple hand tools, but the work takes longer. It may therefore be hard to finish certain aids in a single day. A few power tools, especially an electric jigsaw and an electric drill, can speed things up considerably.
IMPORTANT: I cannot emphasize too much how essential it is that all the necessary tools and materials for the workshop be obtained and ready ahead of time. In the Nicaragua workshops, certain key supplies had still not been obtained by the beginning of the event. In one workshop the lack of an electric jig-saw meant that so much time was lost that the final trails and adjustments were not completed by the time of the final evaluation session. This caused a number of disappointing results that could have been avoided. Similar lack of nails the right size, and of pliers, led to other problems.
Before the workshop begins, some very responsible person should go down the checklists below and be sure all the agreed-upon tools and materials are on hand.
1. Tools Needed
-
pencils with erasers
-
marking pens (thin and thick line, bold colors)
-
yard sticks - or long straight rulers
-
tape measures (one per group)
-
hammers (with claws)
-
screwdrivers
-
pliers, regular and vice-grip
-
set of small hexagon wrenches
-
vices and wood clamps for gripping
-
hand saws
-
metal saw
-
hole saws for plywood
-
manual jig saws
-
electric jigsaw(s) with many extra blades
-
awl (small pointed tool to make holes)
-
hand drill, or brace and bit—with bits
-
electric hand drill and set of bits
-
sharp knives (e.g. linoleum knives)
-
wood chisels
-
hand-held electric sander (if possible)
-
wood rasps
-
metal file
-
wire cutters and tin snips (sheers)
-
strong scissors (at least 3)
-
heat gun (if possible)
-
staple gun with staples (optional)
-
paint brushes (for painting toys)
2. Materials Needed
-
sheets of paper (for writing, drawing)
-
poster paper (large sheets of paper)
-
duct tape
-
electrical tape
-
plywood (1⁄4” and 1⁄2” - 4’ x 8’ sheets)
-
variety of boards and strips of wood
-
nails (1⁄2,” 3⁄4" , 1", 11⁄2", 2" and 3")
-
screws, assorted sizes
-
nuts and bolts, assorted sizes
-
small brads or tacks
-
string (1 and 2 mm thick)
-
baling wire or other thin wire
-
rope ( c and 1⁄4 inch)
-
Velcro (if possible)
-
fast drying glue (2000 o 5000)
-
sheets of foam plastic, 1" and 2" thick
-
sheet foam rubber, fairly dense, 1" thick
-
butcher paper
-
old newspapers
-
colorful cloth (for covering cushions, etc.)
-
old sheets and strips of cloth
-
cotton (for padding and filling)
-
old bed sheet
-
large needles and strong thread
-
old plastic bottles, buckets and tubs
-
old car tires (without wire in walls, if possible)
-
old inner tubes, from cars and bikes
-
sandpaper (fine and course)
-
thin sheet metal, or old metal cans
-
plasticine, Silly Putty, or firm clay (for making individually-shaped handles for holding pencils, spoons, etc.)
-
quick-setting “body putty” (Bondo) for car repair, 1 litre
-
building plaster (plaster of Paris)
-
pieces of leather
-
plastic hose, 1⁄2 to 3⁄4” thick
-
buckles and clasps
-
small bells
-
shiny paper or foil of different bright colors
-
paints: fast-drying non-toxic water-based, bright colors
3. Paper-Based Materials and Preparation
-
corrugated cardboard, large sheets of different thickness, up to 3⁄4" thick
-
white carpenter’s glue, at least 2 liters (see below)
-
old strong paper sacks (used for cement, etc.)
-
old magazines with colorful pages
-
broad paper tape (masking tape)
It is important to prepare ahead for paper-based technology. If aids using paper-based technology are to be made in a single day, it is essential that large, thick sheets of cardboard be laminated at least 2 or 3 days in advance, so that they are dry and strong when needed (see p. 7). If glued several days in advance, a low-cost home-made paste (a runny mix of wheat flour and water) can be used instead of more costly carpenter’s glue.
Open Copyright For Health and For All
As most readers of this newsletter are aware, David Werner’s book Where There Is No Doctor broke new ground in self help health care. The book demedicalized and demystified health information and put the power of knowledge into the hands of people the world over for whom it had previously been out of reach. But before getting to the table of contents, David broke new ground in another arena as well. He “de-legalized” the book with an innovative and progressive open copyright policy, allowing any and all people and groups to copy and adapt the book to their needs and circumstances, as long as it is done on a non-profit basis. This would become the open copyright statement in the front of each and every book by David Werner.
The open copyright statement of every book by David Werner:
Any parts of this book, including the illustrations, may be copied, reproduced, or adapted to meet local needs, without permission from the author or publisher, provided the parts reproduced are distributed free or at cost—not for profit. For any reproduction with commercial ends, permission must first be obtained from the author or the Hesperian Foundation. The author would appreciate being sent a copy of any materials in which text or illustrations have been used.
To understand why David did this, it is important to understand how the book evolved. Where There Is No Doctor, originally written and published in Spanish as Donde No Hay Doctor, grew out of Project Piaxtla in the rural mountains of Western Mexico. It holds within its pages the stories of many whose lives, and sometimes deaths, provide a window into a much larger community. The book was truly a labor of love.
I recently read some early editions of this newsletter, and the following passage from 1971 stood out. David wrote,
A baby is born . . . and begins to fail shortly after birth. An urge deep within us, almost as basic as hunger or lust, demands we do our utmost to save that baby’s life…. The infant deserves to be saved, not because it is living but because it is loved! Love is the ultimate and the only justification for all life and any life, for any and all action. There is no other. None.
(See Newsletter #07 for the full quote in its poetic context.)
It is David’s deep personal connection with the people in his community that inspired all his books, and inspired the open copyright. Even though David was the focal point for the books, the village of Ajoya and the surrounding region contributed immensely to their development. The open copyright printed in the front of each of these books is, in large part, a reflection of what was learned in this community over many years. These books truly belong to the community that spawned them, and to the much larger community of humankind.
Today, David’s books assist health and disability workers in communities around the world save lives and help disabled people regain or increase their capacities, thus their copyrights are a sacred trust. The only real reason to copyright these materials is to maintain their quality, and to assure no one tries to limit access to them.
It is in the spirit of the open copyright that HealthWrights has put all of David’s books in electronic form, and published them on our web site. We realize that for many the Internet remains beyond reach. But more and more, it is becoming a truly world wide web, and disadvantaged people around the world are slowly gaining access.
David initiated the open copyright to help assure that these materials would be available to those who most need them. Since its inception, the open copyright has stood as a model that many other groups around the world have emulated, creating a large body of work that puts the needs of people before profit. Putting David Werner’s books online for all to use is a contemporary expression of the open copyright.
Today there is a thriving open-copyright movement. How much of it has been directly influenced by David’s pioneering example is anyone’s guess.
Current Expressions of Open Copyright
Creative Commons is a nonprofit organization that encourages flexible copyrights for creative works. Their model allows the author of a work to retain their copyright, but offer some rights to anyone who meets certain conditions stipulated by the author. That stipulation may be as simple as getting credit for being the creator of a work, or something more complex such as reproducing a work only on a non-profit basis. And it applies not only to text, but also to pictures, movies, and
sound (music, speeches, etc.). For more information, see: http://creativecommons.org/
We have also seen this extended into software with the copyleft movement. As explained on the “Gnu” website,
Copyleft is a general method for making a program or other work free, and requiring all modified and extended versions of the program to be free as well.
In that way it uses David’s open copyright idea to assure that new innovations remain free and adaptable as well. See: www.gnu.org/copyleft/copyleft.html
Update on PROJIMO
Both of the PROJIMO projects continue to provide greatly needed services for disabled children and adults in Sinaloa Mexico. Run by disabled villagers who have become highly skilled in helping families to meet a wide range of rehabilitation skills, everything from wheelchair making to counseling mothers about early stimulation of children who are developmentally slow.
PROJIMO plays an increasingly important role in sharing its methods and skills with community based rehabilitation programs in other parts of Mexico and Latin America.
Here the team of disabled wheelchair builders in the new workshop in Duranguito teaches 3 disabled persons from the state of Colima how to construct wheelchairs that are individually designed to meet the needs of each child.
Although PROJIMO was originally set up to serve the rural area, many disabled persons come from the cities, because often they can get more personalized and comprehensive services than in the hospitals or large urban rehab centers. An example is Alberto, from Culiacan, the state capital, who is quadriplegic (paralyzed from the neck down).
When Alberto arrived at the PROJIMO community rehab center in Coyotitan he was completely dependent, had severe pressure sores and was so drugged on anti-epileptic medicines (though he didn’t have epilepsy) that he was like a zombie. Once the village team graded him off the medication he became much more alert, and found he could do many more things for himself.
|
|
|
Income Generating Activities
Both PROJIMO programs are trying hard to become as self sufficient as possible. As some of their long-term funding sources are being cut back, they are developing different income-generating activities.
One income generating activity is the intensive conversational Spanish language training course, taught by spinal cord injured young persons. Many of the students both study and volunteer in the rehab program. PLEASE COME STUDY—OR HELP PROJIMO SPREAD THE WORD.
Another income generating activity is PROJIMO’s newly modernized Cyber Café. Fortunately, Jason Weston’s brother Ted, and Stian Haklev from Norway have installed a high speed, satellite-based Internet system which is especially appealing to young persons in the village of Coyotitan.
End Matter
Please Note! If you prefer to receive future newsletters online, please e-mail us at: newsletter@healthwrights.org

| Board of Directors |
| Trude Bock |
| Roberto Fajardo |
| Barry Goldensohn |
| Bruce Hobson |
| Donald Laub |
| Eve Malo |
| Myra Polinger |
| Leopoldo Ribota |
| David Werner |
| Jason Weston |
| Efraín Zamora |
| International Advisory Board |
| Allison Akana — United States |
| Dwight Clark — Volunteers in Asia |
| David Sanders — South Africa |
| Mira Shiva — India |
| Michael Tan — Philippines |
| María Zúniga — Nicaragua |
| This Issue Was Created By: |
| David Werner — Writing, Layout, and Photos |
| Jason Weston — Writing and Layout |
| Monique Elegeert — Photos |
| Trude Bock — Proofreading |
| Bruce Hobson — Proofreading |
Political tags—such as royalist, communist, democrat, populist, fascist, liberal, conservative, and so forth – are never basic criteria. The human race divides politically into those who want people to be controlled and those who have no such desire.
— Robert A Heinlein