












Coping with COVID—The Need for Equality, Inclusion and Global Solidarity
The COVID Pandemic
This last year, with the disastrous COVID-19 pandemic, has been a challenging one worldwide. Massive setbacks in health and livelihoods have accentuated the stark inequities within communities and between countries. Especially in nations with a huge gap between rich and poor, those living in the most disadvantaged conditions have been hardest hit by the virus. Not only do those with the lowest wages live in the most crowded and vulnerable conditions, but typically do the “essential” jobs that increase their exposure to the virus. And they often have preexisting health conditions that increase the morbidity of the virus.
The United States, with an income gap among the world’s widest, has likewise had by far the highest rates of COVID. The US, with only 5% of the global population, soon had over 20% of the world’s cases and deaths from COVID. There are many contributing causes for this, including high-level mismanagement and a maelstrom of misinformation, coupled with systemic racial and class discrimination. In the US, COVID case and death rates among Latinos and Blacks have been two to three times higher than in whites—an inequality led by the glaring disparity of income.
In Mexico, the pandemic has likewise struck disastrously hard—in part for similar reasons. After the US and Brazil, Mexico has among the highest income disparities in the Americas. Although the World Bank now dubs Mexico a “middle-income country” (MIC) thanks to its growing number of multimillionaires, a large swath of the population still lives near or below the poverty line. The living and working conditions of this impoverished underclass make social distancing and other COVID precautions difficult. And widespread distrust of authorities doesn’t help.
In Mexico, as elsewhere, the COVID-provoked unraveling of the economy has also especially devastated the poor, droves of whom have lost jobs as local shops and businesses cut back or close down. Many families we’ve known for decades, who farm or fish for a living, can no longer sell their produce because multitudes are too destitute to buy needed food. Many subsist on a few tortillas, occassionally with a bit of frijoles de olla (diluted bean soup). They can’t pay their electric bills, water bills, or rent. Government assistance to the distressed is at best paltry and hit-or-miss. The numbers of homeless are surging. Suicide has increased. … But at the same time there are many heartwarming examples of folks sharing what little they have and helping each other out.
The continuing pandemic has been has been a big challenge for the disability and rehab programs with which HealthWrights collaborates. Amazingly, both the PROJIMO programs (in Coyotitán and Duranguito) keep on providing much-needed services, despite the difficulties and constraints. Habilítate Mazatlán (the newer program run by disabled recovering drug users)—continues to custom-make special seating for children who need individualized aids. Now in the hard times of COVID, many of the families with ties to these programs involved in are struggling to meet their needs—as are the programs themselves, and HealthWrights is seeking ways to assist.
Where Will the Pandemic Go from Here?
Forecasts of how and how long the COVID pandemic will continue vary widely—from distressingly pessimistic to what I fear is naively hopeful. Over and again, the fateful “curve” of new cases has flattened or dropped, only to be followed by another—and yet another—more ominous surge. Predictions of when the plague will abate and life will return to normal have been repeatedly pushed to later dates.
Hopes (for many but not all) have risen with immunization. Thanks to “warp speed” development of vaccines, optimism (and for anti-vaxxers, pessimism) has rebounded. A fair number of people have already been vaccinated—at least in the richer countries where vaccines are more available. And in some of those same countries, numbers of new cases have begun to drop.
But the wave of optimism may be premature. A combination of factors could set back the gains.
To effectively halt the pandemic, epidemiologists say we need to reach “herd immunity”, i.e., enough people must become immune—by vaccination and/or contagion—so the virus no longer spreads. Herd immunity is attained only after a certain percentage of the population has gained immunity—a percentage that’s higher the more contagious the infection. For COVID-19, epidemiologists estimates herd immunity is achieved when 80% of the population can’t get infected.
But getting to herd immunity is a race against time. As long as large numbers anywhere can still contract the virus, lots of mutant strains will continue to evolve, and it will be more likely that some of the new variants will be more contageous, more deadly, and/or more vaccine resistant. Already ominous variants have appeared in England, South Africa, Brazil—and more recently in California and New York (all regions that have had exceptionally high COVID rates). These new variants are rapidly spreading worldwide. The sooner enough people are vaccinated to achieve herd immunity, the greater the chances of containing the pandemic before it gets totally out of control.
However, these control efforts must be worldwide. The coronavirus respects no boundaries. If the US achieves high vaccination coverage, protection will be short-lived if other places don’t achieve the same. Newly mutated variants may spread even faster and be more deadly, and/or resist the current vaccines. So unless every country reaches adequate coverage, new, more dangerous COVID strains, originating anywhere, may soon spread everywhere. This means the whole world must have the necessary vaccines—and quickly. No nation—however wealthy or heavily armed—is an island unto itself.
Big Pharma—taking bows for its “warp speed” creation of COVID vaccines—is in reality an unconscionable obstacle to achieving high global immunization coverage quickly enough to halt the pandemic. The giant, profit-hungry drug companies—which government (i.e., taxpayers) financed handsomely to develop vaccines in record time—greedily oppose sharing their carefully guarded formulas or waiving their monopolistic patent rights granted them by the World Trade Organization’s international patent agreement, called TRIPS (Trade-Related Aspects of Intellectual Property Rights). An emergency waiver of relevant patent rights during the pandemic—so that billions of vaccine doses could be produced quickly at low cost by multiple qualified non-profits in low and middle income countries (LMICs)—has been petitioned for by the World Health Organization and over 100 member countries. But Big Pharma, backed by a few rich capitalist nations representing 13% of the world population (US, EU, Canada, Japan, Australia, South Korea, et al.) strongly opposes such a potentially life-saving waiver. The big drug companies tout their generosity in pricing their vaccines at “only” about US$20 per dose, whereas normally they would charge at least $600/dose for a newly patented medicine. But even at $20, their profits are substantial. It’s estimated that by waiving the patents, COVID-19 vaccines could be produced rapidly in vast numbers at around $2 per dose—thereby saving trillions of dollars, millions of lives, and preventing immeasurable social and economic distress.
But even during a deadly pandemic, within our unbridled market system it’s profit before people! While hundreds of millions are driven to hunger and homelessness and more than three million have died from COVID as of mid-April 2021, during the pandemic, the world’s 600 wealthiest people have increased their wealth by $1.3 trillion!
Epidemiologists calculate that at the current rate of profitable, patent-protected vaccine production—even with President Biden’s recent call for doubling the output—it could take 5 years to produce sufficient vaccine to immunize enough of the world population to reach the global herd immunity needed minimize the probability of far more dangerous mutations of the virus. To offset the likelihood of inestimable global disaster, the current “free market” policy of patent-and-profit protected production of vaccine is far too slow.
In the US, the economic and social COVID-related costs have been astronomical. As of mid-March 2021, the US government reportedly had spent more than $5.3 trillion … the vast majority for expenses within its own borders. Proportionately very little was spent to help meet the pandemic-related needs in other parts of the world. This self-centeredness is hazardously shortsighted, since the only way to definitively defang the COVID Monster is to achieve worldwide immunity. Public Citizen calculates that with a mere $25 billion (“mere” compared to the trillions already spent in relation to COVID), the US government could provide the 17 billion or so doses of vaccine needed to immunize the whole of humanity. In the long run, such foresight could save millions of lives and trillions of more dollars.
Yet another looming obstacle to achieving adequate herd immunity is “vaccine hesitancy”. Distrust of the COVID vaccines has become increasingly contagious in the US and Europe, but also in Mexico and many other countries, rich and poor. A growing legion of “anti-vaxxers” loudly opposes virtually all vaccines, claiming they are toxic, cause autism in children (repeatedly studied and disproven), or claim that vaccination is a totalitarian ploy to implant monitoring devices in everyone.
Clearly medical errors as well as abuses of authority, overt and covert, exist … and a reasonable degree of caution and distrust makes sense. Many medications occasionally do cause adverse reactions, some more than others. In the past, bad batches of inadequately-attenuated live vaccines have caused paralysis and deaths. Even effective vaccines in very rare instances provoke serious reactions. (e.g., “COVID-19 vaccine and Guillain-Barre Syndrome: Let’s Not Leap to Associations”) However, with most vaccines produced today, stringent precautions are taken. Risks tend to be minimal compared to the enormous benefits. (I give examples, below, of the life-saving impact of vaccines from my own observations in Mexico.) While the COVID-19 vaccines were developed in record time, there is little doubt that great care has been taken with controlled studies and testing. Evidence points strongly to there being very low risk compared to enormous benefits, individually and potentially humanity-wide.
Activities to Help Doubters Weigh the Pros and Cons of Vaccination
In these times of contagious “vaccine hesitancy” much has been written on ways to convince folks to understand the importance of immunization against COVID. A wealth of clear, appealing, easy-to-understand material is currently available in print, in videos, and online. Yet millions still have their doubts.
Distrust of vaccines is nothing new. Long before COVID-19, fear-raising rumors spread by avid “anti-vaxxers” triggered such waves of vaccination refusal that they precipitated resurgence of measles, whooping cough, and polio in lands where they had been all but eliminated. Now, with “infodemics” of misinformation buzzing through the social media, distrust of vaccines has spread so rampantly that it deters the prospects of preventing, through timely “herd immunity”, the likelihood of far worse levels of disaster.
The hazards of such myopic delay are huge! High vaccination coverage, as quickly as possible, is needed to curb the pandemic before dangerous new variants take over. To reach high enough vaccine coverage, it’s important that all of us currently bombarded with “fake news” about vaccines, get accurate information clearly conveyed to them on their turf and terms, so that we can rationally weigh the pros and cons of getting vaccinated.
To come to grips realistically with the pandemic, it’s important that all of us—where possible through our own observations—realize that:
-
the risks from the vaccine are very small compared to catching COVID,
-
getting vaccinated, in addition to personal protection, helps protect the whole of society,
-
only when enough people—worldwide!—get immunized can the spread of the virus be stopped and the pandemic ended.
To reach this collective goal, it’s essential that nearly everyone everywhere collaborate. The choice to get jabbed isn’t just a personal option, but contributes to the well-being of all. This doesn’t mean anyone should be vaccinated by force (an imposition that could soon prove counterproductive). Rather it means everyone should get clear, accurate information, adapted to our various ways of thinking and looking at things, so that we can all make well-considered, evidence-based decisions, for our own good and the common good.
It’s unlikely many avid anti-vaxxers will change their minds. But these inflexible naysayers are relatively few: rarely more than 2.5% of a given population. Yet the seeds of doubt they sow in the minds of the larger public has led much larger numbers—often without giving it much thought—to eschew vaccination. Surveys in the US have shown that “vaccine hesitancy” averages from 20% to 40% of the public. Among care providers in some old-age homes—despite their exceptionally high risk—nearly 60% have refused vaccination! Likewise, polls show that Republicans (political conservatives or devotees of Donald Trump) tend to be far more vaccine-scorning). People of color (Black and brown), though they die from COVID twice as often as whites, tend to be more vaccine-distrustful than are whites (which is understandable given their history of having been used as guinea-pigs in medical research and vaccine trials).
It is therefore essential that ALL OF US—including skeptics and rebels—come to realize that one of the best ways to help ward off cataclysm caused by proliferation of more aggressive mutants is for virtually everyone on earth to get vaccinated against COVID as soon as possible.
This means that ALL OF US—in all walks of life, rich and poor, urban and rural, schooled and unschooled—need the opportunity to thoughtfully consider the facts, look critically for the truth, and recognize misinformation for what it is.
This kind of sobering critical analysis—both personal and collective—calls for what some of us dub “discovery-based learning”. It can help us to think for ourselves, make our own observations, and reach rational decisions for the common good.
Methods for facilitating this sort of liberating, think-for-yourself learning process are explored in Paulo Freire’s eye-opening book, Pedagogy of the Oppressed. Further examples of “discovery-based learning” can be found in our handbook, Helping Health Workers Learn (Werner and Bower, accessible through www.healthwrights.org). A number of these learning tools were developed in intercambios educativos (educational exchanges) with village health promoters from community-based health programs in Mexico and Central America during the 1980s and ’90s.
Use of Street Theater and Participatory Role-Plays to Rethink ‘Vaccine Hesitancy’
Widespread suspicion of vaccination is nothing new to the Mexico’s Sierra Madre, where I helped to launch the community based health program. In the 1960s when the villager-run health program began, the mountain region had disturbingly poor levels of health. Maternal and child mortality were high. One in ten women died in childbirth. One in three children didn’t reach age five. Tetanus (lockjaw) was a common cause of death. Half the women, by the time they reached menopause, had lost at least one baby to neonatal tetanus. The health team managed to lower these deaths by encouraging midwives to use a sterile razor blade to cut the umbilical cord. But not until we finally succeeded in routinely vaccinating pregnant women against tetanus did deaths from neonatal tetanus fall almost to zero.
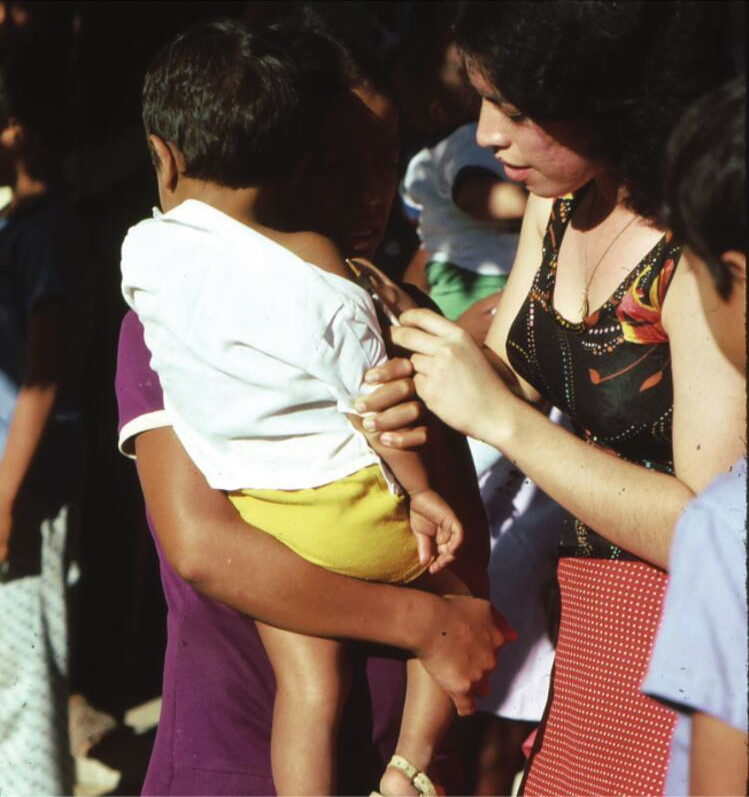
But convincing the villagers that vaccination was important wasn’t easy. In the late 1960s, when we began to immunize the children against polio, tetanus, whooping cough, diphtheria, measles, and tuberculosis—all disabling or deadly diseases in the Sierra Madre at the time—most villagers were hostile toward vaccination. A decade earlier soldiers had marched into the mountains and, with little explanation, jabbed every child they could catch. In those times Mexico still vaccinated against smallpox, as a safety precaution since smallpox had only recently been eradicated worldwide. From the vaccine children became feverish and got a nasty, painful sore on their shoulder. So, understandably, parents got upset. Before the jab their kids were healthy; afterwards they were not. So the campesinos vigorously resisted further vaccination. Then, two years before the Piaxtla program began, a curandero (traditional healer) named Mencho—who understood the life-saving potential of immunization, had obtained vaccines in the county seat and begun to immunize children. But the community angrily protested. One father even threatened to shoot Mencho if he persisted. So he stopped. Since then no one had tried to vaccinate in the back country—until we launched an immunization program in 1967.
By that time, fortunately, many of the villagers had come to appreciate the community health program. When the health promotores explained the purpose of vaccination, some folks—if still a bit hesitant—cooperated. But many not yet. Thus the program’s early vaccination efforts were only partially successful. We managed to vaccinated about half the children. A lot of families remained suspicious and didn’t take their children to be vaccinated … until a tragic event led them to reconsider. It happened like this:
In the small, indigenous village of Guillapa, a few weeks after the health team’s efforts to vaccinate there, a little girl named Xochi suddenly fell ill and died of tetanus. She had not been vaccinated. When her two sisters got the shots, Xochi hid and had gone without. A few weeks afterwards, as it happened, all three sisters got their ears pierced for earrings by their grandmother, all with the same sharp thorn. Four days later, Xochi developed a fever and had trouble opening her mouth. The next day her whole body began to suddenly arch backward with the painful spasms of tetanus. After an excruciating few days, Xochi died. Her two sisters, however, were fine. Word of the little girl’s agonizing death spread through the mountains.
The Piaxtla health promoters, on revisiting the distant village, figured out the chain of causes that had led to the girl’s tragic death. They explained things to the bereaved family, who then deeply regretted not insisting that Xochi get vaccinated along with her sisters. With Xochi’s parent’s consent, the health promoters composed a brief educational skit based on this sad event. When they first presented it in Guillapa, at the end of the skit, the girls’ mother, weeping, told everyone she now realized why Xochi died and why her sisters were spared. She asked her fellow campesinos to draw their own conclusions. There was a lot of discussion and debate. In the end, most agreed that vaccination had likely made the difference. Xochi’s mother begged everyone to get their children vaccinated.
The health promoters performed this brief skit in several of the neighboring villages, followed by open-ended discussions. The skit seemed to mark a turning point in people’s viewpoint and soon led to their energetic support of the vaccination effort. In fact, people of the barrancas eventually became so motivated they began to send mules to the distant Ajoya health center to transport the ice chests with vaccines. And the school teachers, and the schoolkids themselves, diligently spread the word and helped organize vaccination process in their village.
As a result of this popular involvement, vaccine hesitance began to abate. After giving it some thought, many who’d been suspicious of the vaccination campaign began to cooperate and even help promote it. Within five years, coverage in the mountain area became exceptionally high, and the incidence of the infectious diseases of childhood conspicuously declined. Indeed, polio—which had been paralyzing hundreds of children for generations—disappeared from the remote project area of the Sierra Madre almost three years before polio was eliminated from the barrios of the coastal cities.
This kind of collective commitment as seen in the Sierra Madre can be encouraged through an educational process that invites people to think for themselves. The skit—based on a heart-breaking event in their own community—helped people clarify their own observations and make rational decisions to take action for the common good.
Possibilities for facilitating this sort of empowering, people-centered learning process are laid out by Paulo Freire’s in his revolutionary book, Pedagogy of the Oppressed. A potpourri of other “discovery-based” learning tools—developed through decades working with village health promoters in Mexico and beyond—can be found in our handbook, Helping Health Workers Learn.
The Measles Monster
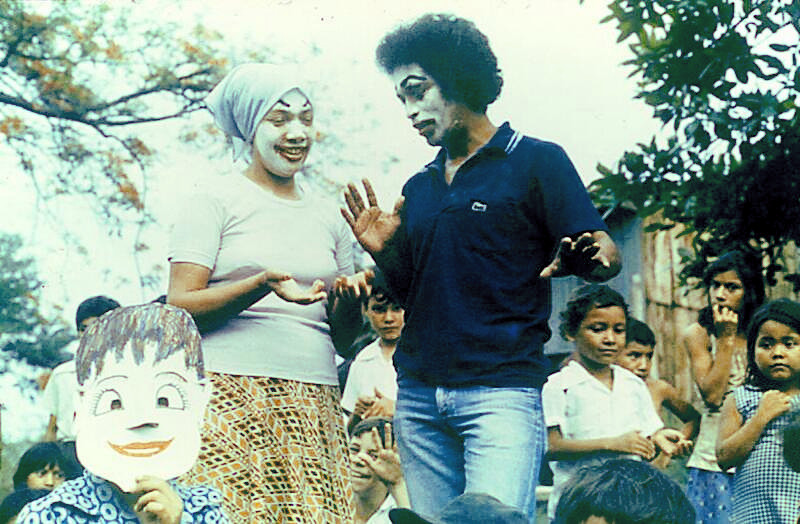
Another example of using participatory drama to confront “vaccine hesitancy” took place in Nicaragua, a few months after the Sandinistas had overthrown the oppressive Samosa government. The country’s new ministry of health (MINSA)—which was familiar with our villager-run health initiative in Mexico—invited a group of us from Project Piaxtla to go to Nicaragua to facilitate a community-based workshop focusing on “health education for change”. The ministry had launched an intensive country-wide vaccination campaign. This national campaign, however, was being surreptitiously undermined by the US Central Intelligence Agency (CIA) which spread rumors that the vaccines would sterilize whoever got them. (As proof, it was pointed out that the little bottles had printed on them, “agua esterilizada”! So lots of people grew “hesitant”—or worse.) To confront this sabotage, as part of our workshop, the participating brigadistas organized a street-theater skit in the marketplace, recruiting passersby and children as actors.
The Measles Monster skit opens with a brigadista (speaking through a narrator with a loudspeaker) loudly announcing the vaccination campaign. But one family (their faces painted white), having heard the worrisome rumors, decides not to vaccinate their children, but instead go to the beach. At that moment the huge, fierce “Measles Monster” (a tall nun played this role) rushes in, chasing after the kids on the street to catch any who are not vaccinated.
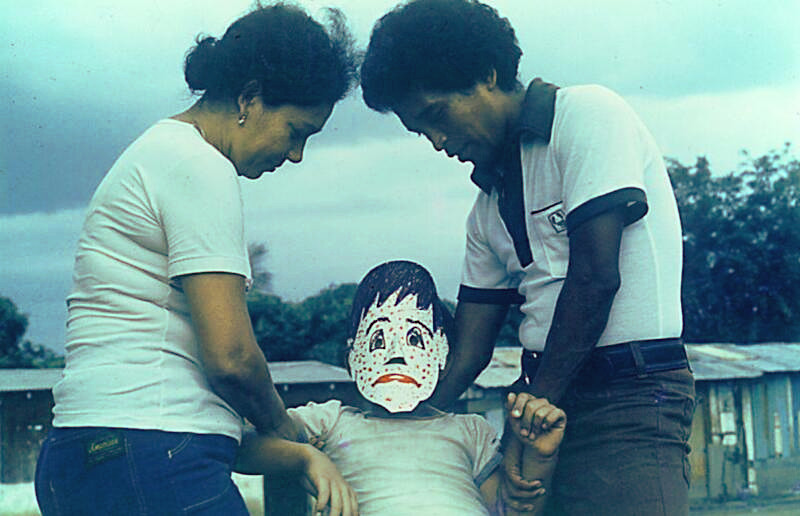
The children flee the Measles Monster in terror. The monster catches a child of the vaccine-hesitant family, enveloping him in its huge claws. When the monster releases him, the boy is wearing a white mask covered with the red dots of measles. He becomes very ill and nearly dies—but at last recovers, with a new mask that’s very pale and thin.
The brigadista reappears, announcing another “day of vaccination”. The boy’s family—having learned the hard way— now eagerly take all their children to be vaccinated. At the skit’s end, the brigadista asks the crowd, “Why did this child get measles?” Everyone shouts, “Because he wasn’t vaccinated!”. Then the brigadista asks, “And now why do none of the kids in this family get measles?” And everyone shouts, “Because they’re all vaccinated!”
As the skit came to an end, the group of children gathered on the street got so charged up that they attacked the Measles Monster, throwing it to the ground. (The nun inside the monster costume actually suffered a few cuts and bruises—but said it was worth it.)
After the skit, more of the locals were supportive of vaccination. Even kids were eager to be jabbed.
The COVID Pandemic as an Alarm Call for Far-Reaching Social Change
The COVID-19 pandemic has made obvious, more clearly than ever, the cruel injustices built into our contemporary political and economic order, the crux of our global systemic pecking order with its wide and growing gap between haves and have-nots. During this pandemic it is the poorer, more disadvantaged people, nationwide and worldwide, who are hardest hit, not just by COVID but by the crushing hardships of job loss, hunger, homelessness, and despair accompanying the claws of the virus. It is those in the most vulnerable in the poorest countries who have the hardest time getting adequate measures of care and of prevention. While the richest nations are hoarding vaccines, as things stand now it may take years before those in the poorer nations get enough of their people immunized to reach herd immunity.
Likewise, the failings of our profiteering market model of medical care and pharmaceuticals has become unconscionably obvious during the pandemic. Poorer countries are rightly demanding a waiver of global laws that, by systemically putting profit before people, are greatly increasing the risk of aggravating and perpetuating the pandemic, globally.
In response to this demand, modest steps have been taken by the powers-that-be to temporarily relax some of the regulations that put the economic growth of the rich above the urgent needs and survival of the poor. With luck, perhaps enough people worldwide will get vaccinated in time to rein in the current pandemic. So, as many say, we can “get back to normal”.
Problem is that “normal”, as we’ve come to know it, is the unfair, unkind, cruelly disequal state of local and global affairs that led to the pandemic in the first place. If we human beings are to avoid far more crushing pandemics in the future, and even more pan-cataclysmic events such as ecological demise, mass starvation, and/or nuclear war—we need more than temporary waivers of laws governing the global marketplace. We need a humane transformation that puts people and nature before profit, and need before greed. Let us be woken by this brutal pandemic to organize and share, and to be kind, beyond national and racial and conventional boundaries, to build a convivial way of living in harmony with all peoples, with all living beings, and with the Gaia, the earth herself. Let us let the pandemic, painful as it’s been, be the birthing process of new life of sharing and caring that embraces diversity and includes all, with empathy and love.
The Measles Monster Slideshow Available Online
Participatory skits and thought-provoking street theater are good ways to engage folks in looking at crucial issues in new ways. Such provocative drama may be especially effective in reaching those millions who live in rural areas or disadvantaged situations with little access to social or mass media.
For this reason we attach here a link to a slideshow of the Measles Monster—in hopes it may give health workers and educators ideas for creating similar skits or puppet shows to mobilize hard-to-reach communities to take part in vaccination campaigns and other activities to help build a fairer, kinder, healthier environment for all.
Feel free to use, copy, or adapt this slideshow in anyway you wish—perhaps as The COVID Monster. If you do use it, please let us know.
One of our current projects is converting about 20 presentations and powerpoints into mobile-friendly versions. Visit also our presentations page to see them.
End Matter

| Board of Directors |
| Barry Goldensohn |
| Bruce Hobson |
| Jim Hunter |
| Donald Laub |
| Leopoldo Ribota |
| David Werner |
| Jason Weston |
| Efraín Zamora |
| International Advisory Board |
| Allison Akana — United States |
| Dwight Clark — Volunteers in Asia |
| Mira Shiva — India |
| Michael Tan — Philippines |
| María Zúniga — Nicaragua |
| This Issue Was Created By: |
| David Werner — Writing, Photographs, and Drawings |
| Jason Weston — Editing and Layout |